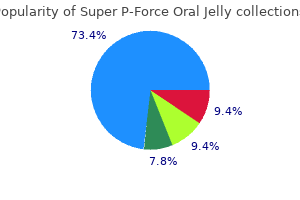
Super P-Force Oral Jelly
Thomas C. Gerber, MD, PhD
- Professor of Medicine and Radiology
- Mayo Clinic College of Medicine
- Rochester, Minnesota
- Consultant in Cardiology
- Mayo Clinic
- Jacksonville, Florida
Nontraumatic chest pain in children and adolescents: Approach and initial management erectile dysfunction treatment phoenix cheap super p-force oral jelly 160 mg with amex. Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents erectile dysfunction age group discount super p-force oral jelly 160mg with mastercard, National Heart erectile dysfunction viagra super p-force oral jelly 160mg discount, Lung impotence and prostate cancer buy super p-force oral jelly 160 mg otc, and Blood Institute erectile dysfunction injection buy super p-force oral jelly online now. Expert panel on integrated guidelines for cardiovascular health and risk reduction in children and adolescents: summary report erectile dysfunction vs impotence order 160mg super p-force oral jelly overnight delivery. Half standard: amplitudes are displayed at half the size; must multiply by 2 to normalize them. There is usually a bimodal distribution, with peaks in the <1 year period, and again during adolescence. Also not tachycardia; can look similar acute bronchiolitis or amenable to ablation often. His breathing is unlabored, there is no hepatomegaly or splenomegaly, and the distal pulses are excellent. A chest X-ray demonstrates clear lung fields and a normal cardiac silhouette, but a narrowed mediastinal shadow. His mother reports that for the last week, he appears hungry, but fatigues with feeds and he now takes twice as long to complete a feeding as he did 1 week ago. Chapter 5: Initial Evaluation of the Newborn with Suspected Cardiovascular Disease; p. The increased oxygen content of blood flowing through the ductus promotes vasoconstriction of the smooth muscle and closure of the ductus. Anatomic Variations Ebstein anomaly develops from the failure of the septal and inferior leaflets of the tricuspid valve to fully delaminate, leading the attachments of the leaflets to be downward (apically) displaced from the annulus, and the leaflets to be abnormal. Since this blood is never oxygenated, leads to worsening cyanosis and decreased cardiac output. If a mother has a bicuspid aortic valve, is a fetal echo indicated during pregnancyfi Tetralogy of Fallot with Pulmonary Stenosis and Tetralogy of Fallot with Absent Pulmonary Valve. Early complete repair of pulmonary atresia with ventricular septal defect and major aortopulmonary collaterals. Usually occurs in isolation, but can be associated with 22q11 deletion or maternal diabetes. By definition the systemic, pulmonary, and coronary circulations arise from one ascending artery. Most have tachypnea, tachycardia, diaphoresis, and poor feeding as severe pulmonary overcirculation develops. In this, the majority of the conus sits below the aortic valve, pushing it anteriorly and superiorly, and the small amount of conus below the pulmonary valve causes it to slightly override the ventricular septum. In this lesion, there is more conus tissue underneath the pulmonary valve, but still enough under the aortic valve to push it rightward, though not anterior. Requires ductus arteriosus for systemic blood flow and is fatal without prostaglandin therapy and subsequent surgical palliation. Anatomic variations and clinical presentation Spectrum of lesions involving pulmonary atresia with variable degrees of hypoplasia of the right ventricle and anomalies of the coronary arteries. Inlet portion of the right ventricle is absent and often there is a dimple in the floor of the right atrium where the valve would have been. If there are normally related great arteries, this causes pulmonary obstruction and increasing hypoxemia. If patients have pulmonary atresia, may show diminished lung markings, or if unobstructed, may have pulmonary edema. There is obligate right to left flow at the atrial septum in order to allow for any blood to enter the left ventricle and provide cardiac output. Semilunar valve Replacement with Decellularized Homograft after Damus Kaye-Stansel Anastomosis and Fontan Procedure. Rastelli operation, 1969 Originally used for transposition of the great arteries, now used for numerous complex repairs, including truncus arteriosus. The two most common cardiomyopathies in pediatric patients are Hypertrophic Cardiomyopathy and Dilated cardiomyopathy, so those are discussed here. For further information on other types of cardiomyopathies, see the References section. Hypertrophic Cardiomyopathy Most frequently occurring cardiomyopathy (1:500 of general population) and has an autosomal dominant pattern of inheritance. Most common cause of sudden cardiac death in young people and competitive athletes. Subtle diastolic changes can be appreciated before objective hypertrophy with careful echocardiography. Ventricular tachycardia and fibrillation can occur in patients without significant obstruction and cause sudden death. Contemporary definitions and classification of the cardiomyopathies: an American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: Task Force 3: hypertrophic cardiomyopathy, arrhythmogenic right ventricular cardiomyopathy and other cardiomyopathies, and myocarditis. International Society for heart and Lung Transplantation: Practice Guidelines for Management of heart Failure in Children. Evaluation, Risk Stratification and Management of Pulmonary Hypertension in Patients with Congenital Heart Disease. Endocarditis: infection of the endocardial surface of the heart, including native or prosthetic heart valves, septal defects, the mural endocardium, foreign devices or patches, surgical shunts and indwelling central venous catheters. They often do not have fever and may present with only generalized sepsis or focal neurologic findings from emboli to the brain. Clinical manifestations and evaluation of adults with suspected native valve endocarditis. Prevention of Infective Endocarditis: Guidelines from the American Heart Association. Revision of the Jones Criteria for the diagnosis of acute rheumatic fever in the era of Doppler echocardiography: a scientific statement from the American Heart Association. Diagnosis, Treatment and Long-Term Management of Kawasaki Disease: A statement for health professional from the committee on rheumatic fever, endocarditis and Kawasaki disease, Council on Cardiovascular Disease in the Young, American Heart Association. Explain branchial apparatus, pharyngeal arch, pharyngeal pouch, and pharyngeal groove (cleft) 2. Explain the embryological basis of: ectopic thyroid gland, branchial cysts, clefts of the lip and palate, thyroglossal duct cyst and sinus Lecture Notes: 1. Recall the layers of the trilaminar embryo: o ectoderm (outside) o mesoderm o endoderm (inside) 2. During weeks 5-8 inclusive (embryo period), the structures of the head and neck are developed. Tissue prominences (Pharyngeal Arches) develop in the location of the primordial neck. This development results from the infiltration of neural crest cells from the head into the mesodermal tissue of the neck. The processes involved in the formation of the pharyngeal arches and their products are (as always) proliferation and selective control of the initiating factor (neural crest cells) into specified locations (Hox genes), followed by differentiation of the mesoderm (Hox genes) into tissue types. These pharyngeal arches (numbered 1,2,3,4 (-6) are separated from each other by an internal (endodermal) pouch and an external (ectodermal) groove. The arches, grooves, and pouches have distinct roles although not each results in the formation of an adult structure. The arches supply the cranial nerves, cartilage and bone, muscles, and ligaments to structures in the head and neck (see Table 10-1, pg 221) st 7. Remaining grooves are nd obliterated by overgrowth of 2 arch during neck development. Invagination of tissue leads to formation of thyroglossal duct (remnant is foramen cecum) c. Know the etiology, presentation and management of pharyngitis, acute tonsillitis and peritonsillar abscess 2. They sit in the tonsillar fossa bordered by three muscles and separated from the lateral pharyngeal wall by connective tissue. The fascial planes play a role in both confining and providing potential routes of spread of these infections. These infections typically develop as a result of tonsillitis, dental infection or salivary gland infection. These patients are usually severely ill and may develop upper airway obstruction due to laryngeal edema. Lococorten-Vioform, Gentian violet / mycostatin powder) Chronic Otitis Externa pruritis without obvious infection use topical corticosteroid alone Malignant (Necrotizing) Otitis Externa Osteomyelitis of the temporal bone that occurs in immunocompromised patients or diabetics. Involvement of the sinus cavities along with the nasal cavity is termed rhinosinusitis. Acute sinusitis is usually secondary to rhinitis (such as that caused by the common cold or influenza), of dental origin or from infected material directly entering the sinus. Treatment is primary medical (decongestants and antibiotics) although occasionally surgical drainage is necessary. Allergic rhinitis displays the clinical triad of nasal congestion, rhinorrhea and sneezing. The response is IgE mediated and requires immunologic sensitization to an allergen. The disorder tends to cluster with other allergic disorders and has a strong family tendency. Our involvement with these children and their families often begins before birth and can extend into late adulthood. Affected individuals present a multiplicity of problems and effective management involves a wide range of specialists. The currently accepted model for delivery of this care in the most appropriate way is the multidisciplinary cleft team. It has been suggested that such an integrated system of delivery of care enables the individuals within the team to function in an interdisciplinary way so that all aspects of health care for the cleft condition can be delivered in as seamless a way as possible. This model has an international acceptance and many centres have slowly developed their services along these lines. It is understood that the antenatal diagnosis of clefts involving the lip is relatively straightforward for an experienced sonographer whereas identification of clefts involving the palate is much more difficult. The needs of children with clefts involving the palate, whether or not the lip is involved, are similar and we shall discuss all types of common labiopalatine clefting. This review is written by and based upon the experiences of the individual specialists working at the Newcastle site of the Northern and Yorkshire Cleft Lip and Palate Service.
Glomerular diseases Kidney International Supplements (2018) 8 erectile dysfunction diagnosis treatment order super p-force oral jelly 160mg without prescription, 91fi165 137 chapter 5 Whether this corresponds to a true association or are not markedly different from the usual reasons prompting a coincidence is unclear erectile dysfunction at age 17 buy 160 mg super p-force oral jelly. The clinical presentation icd 9 code of erectile dysfunction buy super p-force oral jelly master card, outcome erectile dysfunction drugs in philippines buy super p-force oral jelly 160 mg amex, 294 a kidney biopsy for other glomerular diseases erectile dysfunction treatment testosterone replacement purchase 160 mg super p-force oral jelly amex. In addition impotence losartan potassium super p-force oral jelly 160 mg sale, the histology will provide and granular deposits of IgG, IgA, and C3. Viral 303 basement membrane, and accumulation of eosinophilic antigens have been found by immunohistochemistry, in 303 304 material representing precipitated immune complexes or situ hybridization, and laser capture microdissection. The glomerular basement membrane often shows double contours, which are caused by the interposition 5. Both subendothelial and mesangial associated glomerular disease has been provided by a meta immune complexes can be identified by electron microscopy analysis of comparative studies of various study designs 138 Kidney International Supplements (2018) 8, 91fi165 Around 10% of patients present oliguric 330,331 a total of 36 reports based on 47 unique patients were kidney failure. The exacerbation of extrarenal symptoms often remission of glomerular lesions; this cannot be excluded in is associated with a fiare-up of kidney disease, but can occur 318 a few cases. First, the impact of antiviral therapy on the long Given that remission of hematuria, proteinuria, and term outcomes of kidney disease remains uncertain. Potential regimens include ritux immunosuppression concurrent with antiviral therapy. According to the decision of the clinician, immuno by week 4 and remained undetectable while on treatment. Other showing severe disease manifestations, such as progressive case reports have also documented improvement following the glomerular disease. No other immunosuppressive should be administered to achieve recommended target blood drugs were used. Re-induction with rituximab was carried large-sized studies with appropriate technology to assess the out in 9 patients who relapsed after a mean of 31. Kidney International Supplements (2018) 8, 91fi165 141 methods for guideline development The guideline consists of expertise in nephrology and evidence-based clinical practice guide recommendation statements, rationale text, and a summary of sys line development, and experienced research associates. Discussing process, methods, and results Developing and refining topics Establishing the process for guideline development. The Work Group took the primary role of writing and Screening abstracts and retrieving full-text articles on the basis of grading the recommendation statements and rationales and retained pre-defined eligibility criteria final responsibility for their content. Tabulating data from individual studies into summary tables Grading quality of evidence for each outcome across studies, and Formulating questions of interest. The Work Group ranked outcomes of Sending the guideline draft for public review in February 2017 interest on the basis of their importance for informing clinical de Editing the guideline cision making (Table 9). Publishing the final version of the guideline Literature searches and article selection. For new topics, searches were not limited by meetings to finalize review topics, review the available evidence, publication date. The full literature search strategies are provided in formulate recommendation statements, evaluate the quality of the Supplementary Appendix A. Kidney International Supplements (2018) 8, 91fi165 143 methods for guideline development Evidence profiles were constructed to assess relevance and consensus among reviewers, the entire team screened the quality and record quality grades and descriptions of effect (or and achieved consensus on a series of initial batches of 100 abstracts. Journal articles reporting original to make the evidence synthesis process transparent. Decisions in the data or systematic reviews were selected for evidence review, based evidence profiles were based on data from the primary studies listed on a priori criteria for eligible evidence. Extracted data from each study was reviewed by another and then reviewed, edited, and approved by the Work Group. Methodology and out comes were also systematically assessed for risk of bias (see the Grading of quality of evidence for outcomes of individual section on risk of bias assessment below) and recorded during the studies. Data were extracted into the online re design, conduct, and reporting of outcomes of a clinical study. Summary tables were developed for each done by one of the reviewers, then confirmed by another, with reviewed topic. Summary tables contain outcomes of interest, rele discrepancies discussed in conference. Categorical outcomes and continuous outcomes were 351 Cochrane risk of bias tool, which asks about risk of selection bias, tabulated separately. Summary tables are available as selected questions from the Newcastle Ottawa Scale about compa supplementary material at Kidney International Supplements (2018) 8, 91fi165 145 methods for guideline development Fair quality Moderate risk of bias, but problems with study or paper are unlikely to cause major bias. D Very low the estimate of effect is very uncertain, and often will be far from the truth. Based on these Grading the quality of evidence for each outcome across characteristics an overall assessment was made whether the study studies. For each outcome, the potential grade for the quality of vidual grade depending on the quality of reporting and methodo evidence for each intervention-outcome pair started at high but was then logical issues specific to that outcome. However, the quality grade of lowered if there were serious limitations to the methodological quality of an individual outcome could not exceed the quality grade for the the aggregate of studies, if there were important inconsistencies in the overall study. The final grade the quality of the overall evidence and the strength of recommen for the quality of the evidence for an intervention-outcome pair could be dations. For each topic, the discussion on grading of the quality of one of the following 4 grades: high, moderate, low, or very low (Table 12). The refers to the extent to which our confidence in an estimate of effect is resulting 4 final categories for the quality of overall evidence were A, sufficient to support a particular recommendation. Each patient needs substantial debate and involvement of recommended course of action, help to arrive at a management decision stakeholders before policy can be but many would not. The ungraded recommendations are generally written as simple declarative statements. They should not be interpreted as being weaker recommendations than Level 1 or 2 recommendations. Table 16| Determinants of strength of recommendation Factor Comment Balance between desirable and the larger the difference between the desirable and undesirable effects, the more likely a strong undesirable effects recommendation is warranted. Quality of the evidence the higher the quality of evidence, the more likely a strong recommendation is warranted. Values and preferences the more variability in values and preferences, or the more uncertainty in values and preferences, the more likely a weak recommendation is warranted. Values and preferences were obtained from the literature where possible or were assessed in the judgment of the Work Group where robust evidence was not identified. Assessment of the net health benefit across all important clinical feedback, it was further revised by the Work Group Co-Chairs and outcomes. All Work Group members provided feedback on initial the anticipated balance of benefits and harms across all clinically and final drafts of the recommendation statements and guideline text important outcomes (Table 14). Recommen However, Table 16 shows that the strength of a recommendation is dation statements were revised in a multistep process during face-to determined not only by the quality of the evidence but also by other, face meetings and by subsequent drafts by e-mail. Formal decision analyses including cost analysis were not the final draft was sent for external public review. Kidney International Supplements (2018) 8, 91fi165 147 methods for guideline development Overview material Provide a structured abstract that includes the See Abstract and Methods for Guideline Development. Indicate any alternative preventative, including both dialysis and transplant populations. Financial disclosures of Work Group members are Disclose potential confiict of interest. Evidence collection Describe the methods used to search the scientific Topics were triaged either to (i) systematic review, (ii) literature, including the range of dates and databases systematic search followed by narrative summary, or searched, and criteria applied to filter the retrieved (iii) narrative summary. Screening criteria for this and other topics are outlined in the Methods for Guideline Development chapter. The search was updated through May 2017 and supplemented by articles identified by Work Group members through July 2018. Recommendation Describe the criteria used to rate the quality of Quality of individual studies was graded in a 3-tiered grading criteria evidence that supports the recommendations and the grading system (see Table 11). Quality of evidence system for describing the strength of the and strength of recommendations were graded recommendations. Method for Describe how evidence was used to create For systematic review topics, summary tables and synthesizing evidence recommendations. Prerelease review Describe how the guideline developer reviewed and/ the guideline had undergone external public review or tested the guidelines prior to release. Update plan State whether or not there is a plan to update the the requirement for an update will be assessed guideline and, if applicable, an expiration date for this periodically from the publication date or earlier if version of the guideline. Such evidence might, for example, lead to changes to the recommendations or may modify information provided on the balance between benefits and harms of a particular therapeutic intervention. Definitions Define unfamiliar terms and those critical to correct See Abbreviations and Acronyms. Recommendations and State the recommended action precisely and the Each guideline chapter contains recommendations for rationale specific circumstances under which to perform it. Each Justify each recommendation by describing the recommendation builds on a supporting rationale linkage between the recommendation and its with evidence tables if available. Indicate the quality of evidence recommendation and the quality of evidence are and the recommendation strength, based on the provided in parenthesis within each recommendation. Potential benefits and Describe anticipated benefits and potential risks the benefits and harm for each comparison of harms associated with implementation of guideline interventions are provided in summary tables and recommendations. The estimated balance between potential benefits and harm was considered when formulating the recommendations. Algorithm Provide (when appropriate) a graphical description of Algorithms were developed where applicable (see the stages and decisions in clinical care described by Chapters 2 and 4). Implementation Describe anticipated barriers to application of the these recommendations are global. Provide reference to any auxiliary the guideline are anticipated to facilitate documents for providers or patients that are intended implementation and appropriate care. Suggest review criteria were not suggested because implementation with for measuring changes in care when the guideline is prioritization and development of review criteria have implemented. Most recommendations are discretionary, requiring substantial discussion among stakeholders before they can be adopted as review criteria. The decision whether to convert any recommendations to review criteria will vary globally. Research recommendations were also outlined to address current gaps in the evidence base. This category was designed to allow the Work statements may be considered to be relatively strong recommenda Group to issue general advice. Typically an ungraded statement tions; they should not be interpreted as weak recommendations meets the following criteria: it provides guidance based on common based on limited or poor evidence. Common examples include sense; it provides reminders of the obvious; and it is not sufficiently recommendations about frequency of testing, referral to specialists, specific to allow for application of evidence to the issue and therefore and routine medical care. We strove to minimize the use of ungraded it is not based on systematic evidence review. Kidney International Supplements (2018) 8, 91fi165 149 methods for guideline development The Work Group took on the primary role of writing the Hand searches of journals were not performed, and review articles recommendations and rationale statements and retained final re and textbook chapters were not systematically searched. However, any important studies known to domain experts that were missed by Format for guideline recommendations. Each chapter contains 1 or the electronic literature searches were added to retrieved articles and more specific recommendations. Similarly, Supplementary Appendix B Important key points and research recommendations suggesting demonstrates the level of concurrence with which this guideline future research to resolve current uncertainties are also outlined at corresponds to the Institute of MedicineOs standards for systematic 348,349 the conclusion of each chapter. Jadoul trained in internal medicine councilor for the American Society of Transplantation and and nephrology under the mentorship has had a long-standing interest in viral hepatitis and organ of Professor Charles van Ypersele de transplantation. He has served as chair at the Internal Association for the Study of Liver Disease in 2004 Department of Nephrology of the and received the Charles Trey Award from the American Liver Cliniques Universitaires Saint-Luc Foundation in 2001. Jadoul has co-authored over 230 scientific papers, most of University Hospital in Valencia, them published in major nephrology journals. He is currently Spain, and professor of medicine at serving as a theme editor of Nephrology Dialysis Transplantation, the University of Valencia. She is also an active committee member for several Merck Sharp & Dohme Otsuka, Roche national and international hepatology and liver trans Speaker: AbbVie, Amgen, Menarini, Merck Sharp & Dohme, plantation societies.
In untreated respiratory acidosis haustive laboratory analyses erectile dysfunction from anxiety order line super p-force oral jelly, but delirium and with coma erectile dysfunction early 20s generic 160 mg super p-force oral jelly amex, the serum pH is low (less than 7 erectile dysfunction caused by herniated disc generic 160mg super p-force oral jelly with amex. Acid loss in the urine: increased distal Nafi delivery in presence of hyperaldosteronism C erectile dysfunction medications generic super p-force oral jelly 160mg amex. Severe terion that clinically distinguishes between respiratory acidosis of any origin is best treated metabolic and structural disease impotence lack of sleep buy genuine super p-force oral jelly. The presence Multifocal impotence of organic origin order cheapest super p-force oral jelly and super p-force oral jelly, Diffuse, and Metabolic Brain Diseases Causing Delirium, Stupor, or Coma 193 of preserved pupillary light refiexes, despite and more active on the right with bilateral extensor concomitant respiratory depression, vestibulo plantar responses. No decorticate or decerebrate ocular caloric unresponsiveness, decerebrate responses could be elicited. Conversely, if asphyxia, anticholinergic later she awoke, at which time her eye movements or glutethimide ingestion, or pre-existing pu were normal. Four days later she again drifted into pillary disease can be ruled out, the absence of coma, this time with the eyes in the physiologic pupillary light refiexes strongly implies that the position and with sluggish but full oculocephalic disease is structural rather than metabolic. She died on the sixth hospital day with Pupils cannot be considered conclusively severe hepatic cirrhosis. Infrared pu ning, but the later autopsy confirmed the clinical pillometry is more reliable than the fiash impression that these focal abnormalities were 38 light. Ciliospinal refiexes are less reliable than due to her liver failure, not a structural lesion. The light refiexes but, like them, are usually pre initial conjugate deviation of the eyes downward served in metabolic coma even when motor and and slightly to the right had suggested a deep, respiratory signs signify lower brainstem dys right-sided cerebral hemispheric mass lesion. At autopsy, no intrinsic cerebral pathologic lesion was found to explain the abnormal eye the eyes usually rove randomly with mild met movements. We have observed transient down abolic coma and come to rest in the forward ward as well as transient upward deviation of the position as coma deepens. Conju stimulation often provides valuable informa gate downward gaze, or occasionally upward tion about the depth of coma in patients with gaze, can occur in metabolic as well as in struc metabolic disease. The ocular response to pas tural disease and by itself is not helpful in the sive head movement is less reliable than the 39 caloric test, as absence of oculocephalic re differential diagnosis. If caloric stim A 63-year-old woman with severe hepatic cir ulation evokes nystagmus, cerebral regulation rhosis and a portacaval shunt was found in coma. The pupillary diameters were 4 mm on ously deviate downward following lateral devia 39 the right and 3 mm on the left, and both reacted to tion, one should suspect drug-induced coma. Her eyes were deviated conjugately down Finally, if caloric stimulation repeatedly pro ward and slightly to the right. Oculocephalic re duces dysconjugate eye movements, structural sponses were conjugate in all directions. Her mus brainstem disease should be suspected (but see cles were fiaccid, but her stretch refiexes were brisk Chapter 2). There was no history of previous illness, but her parents stated that she had severe emotional problems. She appeared to be A 60-year-old man was found in the street, stu asleep when left alone, with quiet shallow respi porous, with an odor of wine on his breath. After but appeared to resist passive elevation of her assessing radiographically for cervical spine in eyelids. The urine toxicology screens were positive for barbi liver was palpably enlarged. He responded to turates, and she awoke the next morning and ad noxious stimuli only by groaning. There was no mitted ingesting a mixture of sedative drugs to response to visual threat. However, tonic movement elicited full conjugate ocular move deviation of the eyes in response to cold caloric ments. The corneal refiexes were decreased but irrigation signified that normal cerebral control of present bilaterally. He did not move her unresponsiveness was the result of organic, but spontaneously, but grimaced and demonstrated probably toxic or metabolic, and not structural extensor responses to noxious stimuli. Toxicology screening discov muscles were symmetrically rigid and stretch re ered at least one cause, but drug overdosages are fiexes were hyperactive. The plantar responses often mixed, and not all of the components may be were extensor. Patients with metabolic brain disease generally the following morning he responded appropri present two types of motor abnormalities: (1) ately to noxious stimulation. Hyperventilation had nonspecific disorders of strength, tone, and re decreased, and the extensor posturing had dis fiexes, as well as focal or generalized seizures, appeared. Diffuse rigidity, increased deep tendon and(2)certaincharacteristicadventitiousmove refiexes, and bilateral extensor plantar responses ments that are almost diagnostic of metabolic remained. The general autopsy disclosed severe hepatic cir Diffuse motor abnormalities are frequent in rhosis. Paratonia and snout, suck, or grasp refiexes may Comment: In this patient, the signs of liver dis be seen in dementia, as well as in patients in ease suggested the diagnosis of hepatic coma. With increasing brainstem depres first, however, anisocoria and decerebrate rigidity Multifocal, Diffuse, and Metabolic Brain Diseases Causing Delirium, Stupor, or Coma 195 hinted at a supratentorial mass lesion such as carotid distribution infarction initially. However, hypogly cemia also can cause unconsciousness as well as Focal weakness is surprisingly common with focal signs in conscious patients. Others have re have either focal or generalized seizures that 40,41 ported similar findings. He received 35 units of protamine zinc insulin each morning in addition to 5 units of regular in Motor Abnormalities Characteristic sulin when he believed he needed it. One week of Metabolic Coma before admission he lost consciousness transiently upon arising, and when he awoke, he had a left Tremor, asterixis, and multifocal myoclonus are hemiparesis, which disappeared within seconds. His entire left side was the tremor of metabolic encephalopathy is numb and paralyzed. His pulse was 80 per min coarse and irregular and has a rate of 8 to 10 ute, respirations 12, and blood pressure 130/80 per second. The general physical examination was rest and, when present, are most evident in the unremarkable. There was supranuclear left ors may spread to the face, tongue, and lower facial paralysis and left fiaccid hemiplegia with extremities, and frequently interfere with pur weakness of the tongue and the trapezius muscles. It is not seen in patients with uni was given 25 g of glucose intravenously and re lateral hemispheric or focal brainstem lesions. Today, Asterixis was originally described as a sudden fingerstick glucose testing would have occurred palmar fiapping movement of the outstretched 44 much earlier, often before reaching the hospital, hands at the wrists. Incipi abolic tremors it sometimes becomes difficult ent asterixis comprises a slight irregular tremor to distinguish between intense asterixis and of the fingers, beginning after a latent period of myoclonus, and there is some evidence that the 2 to 30 seconds that is difficult to distinguish two types of movements represent the same from the tremor of metabolic encephalopathy. Asterixis is generally seen in awake an irregular oscillation of the fingers, usually in but lethargic patients and generally disappears the anterior-posterior direction but with a ro with the advent of stupor or coma, although tary component at the wrist. The second con occasionally one can evoke the arrhythmic con sists of random movements of the fingers at the traction in such subjects by passively dorsi metacarpal-phalangeal joints. Asterixis can also be elicited tern becomes more and more marked as the pa in stuporous patients by passively fiexing and 46 tient holds his or her wrist dorsifiexed until fi abducting the hips. Flapping abduction nally the fingers lead the hand into a sudden adduction movements occurring either syn downward jerk followed by a slower return to chronously or asynchronously suggest meta the original dorsifiexed position. Electromyograms recorded dur feet is often an easier posture for obtunded ing asterixis show a brief absence of muscular patients to maintain). Ventila nonrhythmic, nonpatterned gross twitching in tory patterns, with the exception of psychogenic volving parts of muscles or groups of muscles hyperventilation, are normal. However, it tion, with nystagmus having a quick phase away may be seen in some waking patients with neu from the side of ice water irrigation; there is rodegenerative disorders. In some patients with psychogenic coma, orders (Creutzfeldt-Jakob disease and related the eyes deviate toward the ground when the 49 disorders). Most conscious bolic brain disease have diffusely abnormal patients with metabolic brain disease are con motor signs including tremor, myoclonus, and, fused and many are disoriented, especially for especially, bilateral asterixis. The patient with cannot concentrate well and cannot easily re gross structural disease, on the other hand, tain new information. Early during the illness, generally has abnormal focal motor signs and the outstretched dorsifiexed hands show irreg if asterixis is present, it is unilateral. Co awake patients with psychogenic illness, if they matose patients with metabolic brain disease will cooperate, are not disoriented and can re usually suffer from partial dysfunction affect tain new information. If they seem disoriented, ing many levels of the neuraxis simultaneously, they are disoriented to self. However, although the overall me tabolism of the brain is relatively constant, dif Earlier chapters of this book have described the ferent areas of the brain metabolize at differ 55 physiologic relationships among the brainstem, ent rates, depending on how active an area is. The produce rapidly evolving neurologic abnor brain suffers a special vulnerability in that it malities. These considerations are central to an maintain their membrane potentials, synthe understanding of many of the metabolic en size and store transmitters, manufacture axo cephalopathies, and the following paragraphs plasm, and replace their always decaying struc discuss them in some detail. Astrocytes also participate in con scanning reveal that this apparent uniformity 52 trolling blood fiow and in maintaining the masks a regionally varying and dynamically fiuc 54 blood-brain barrier. Furthermore, many of the matter, for example, is normally three to four 55 enzymatic reactions of both neurons and glial times higher than in white matter. At glutamatergic synapses, presynaptically released glutamate depolarizes postsynaptic neurons by acting at specific receptor subtypes. The action of glutamate is terminated by an efficient glutamate uptake system located primarily in astrocytes. Lactate, once released by astrocytes, can be taken up by neurons and serves them as an adequate energy substrate. So far, the na ture of the local stimulus to such pathologic vasodilation also has eluded investigators. The effects of the process, however, can act to in crease the bulk of the involved tissue and thereby accentuate the pathologic effects of compartmental swelling in the brain, as dis cussed in Chapter 2. This delayed response may refiect the rela tively slow adaptation of the tonic contractile state of vascular smooth muscle rather than a true uncoupling of fiow and metabolism. A functional magnetic resonance imaging reduces tissue fiow below metabolic needs, is scan of the normal individual fiexing and extending his an uncommon phenomenon limited largely to fingers. Blood fiow increases to a greater degree than oxygen consumption in the motor areas, leading to an arteries at the base of the brain. The paramagnetic oxyhemo cal surgical trauma as well as with subarach globin causes an increased blood oxygen level-dependent noid bleeding and sometimes with meningitis signal in the motor cortex bilaterally. As noted earlier in this volume, however, Several pathologic states of brain are marked unless some primary abnormality of brain tissue by a disproportionately high rate of local blood acts to increase regional vascular resistance, an fiow in relation to metabolism. Ions (Hfi and Kfi) contribute to the extracellular currents that are associated with synaptic transmission. In astrocytes, the [Ca2fi] increase is produced by activation of metabotropic glutamate receptors (mGluRs) and by propagation of Ca2fi waves from neigh boring astrocytes through activation of purinergic receptors (P2Y) or entry of 1P3 (inositol (1,4,5)-triphosphate) through gap junctions. Spatial buffering currents in astrocytes release Kfifrom perivascular end-feet, where Kficonductance is greatest (Kfi siphoning). Flows of 18 mL can fusion required to maintain the vitality of the be tolerated for several hours without leading tissueinmanisnotknown. In net metabolic terms, each 100 g of brain Anaerobic metabolism produces large amounts in a normal human being utilizes about 0. This net fig calcium levels, and the formation of free radi ure, however, hides the fact that glucose con 63 cals, all of which can cause cellular death. Hy sumption in local regions of the brain varies poglycemia (see below), by increasing lactate widely according to local functional changes. Ce neurons probably utilize lactate produced from rebral acidosis is a potent vasodilator, as is glucose by astrocytes when stimulated with 66 potassium, which leaks into the brain extra glutamate. These substances provide increased endothelial-derived relaxing factor), adenosine fuel to the brain when beta-hydroxybutyrate, (probably working through nitric oxide), and acetoacetate, and other ketones increase in the 59,64 prostaglandins (for a review see). For One might question why this is so since it is unknown reasons, however, the brain does not known that slices of cerebral cortex in vitro can appear able to subsist entirely on ketone bod utilize a variety of substrates, including fatty ies, and as mentioned below, some investiga acids and other compounds, to synthesize ace tors believe that ketones contribute to the neu toacetate for entry into the citric acid cycle. The answer appears to lie in the specialized Under normal circumstances, all but about properties of the blood-brain barrier, which, by 15% of glucose uptake in the brain is accounted rigorously limiting or facilitating the entry or for by combustion with O2 to produce H2O egress of substances to and from the brain, and energy, the remainder going to lactate pro guards the narrow homeostasis of that organ. The brain contains about 1 mmol/kg Glucose is transported across the blood-brain of free glucose in reserve and a considerable barrier by a carrier-mediated glucose trans amount of glycogen, perhaps as high as 10 porter (Glut-1).
Syndromes
- An occupational therapist can show you ways to ease pain and swelling and stop the syndrome from coming back.
- Hearing problems or loss
- Begins gaining skills for team sports (soccer, T-ball, etc.)
- Profuse sweating, moist skin
- Fish (older children and adults)
- Blood oxygen saturation (pulse oximetry)
- Is rare during exercise, but may be triggered by rest after exercise
- Iodine overload
- Burns
- Inner ear (cochlear) implants
Magnetic stirrers are installed at the measurement position and subsequent measurement position to thoroughly agitate the samples prior to measurement erectile dysfunction 34 year old male 160mg super p-force oral jelly for sale. By swabbing erectile dysfunction otc meds order cheap super p-force oral jelly, the carbon in attached residues fi Simply change the onscreen settings to switch between aqueous sample measurement specific size autosampler vials required with other systems erectile dysfunction protocol discount discount 160 mg super p-force oral jelly with amex. In addition to aqueous samples erectile dysfunction and pregnancy buy 160mg super p-force oral jelly visa, carbon measurements can also be performed on soil erectile dysfunction protocol food lists purchase generic super p-force oral jelly online, sludge vasculogenic erectile dysfunction causes buy generic super p-force oral jelly from india, sedimentation, and other Water sample can be measured directly in the collection bottles and thus do not need to be transferred to solid samples. Example of sample consumption: Standard specifications: 8 mL/3 measure 638-59328 ments fiUsing this kit: 5 mL/3 measurements. Third-party trademarks and trade names may be used in this publication to refer to either the entities or their products/services. Shimadzu disclaims any proprietary interest in trademarks and trade names other than its own. Shimadzu does not assume any responsibility or liability for any damage, whether direct or indirect, relating to the use of this publication. Health Plan Features Deductble Optons $1,000, $2,500, $5,000 Coinsurance Optons 80/20, or 100/0 Coverage Period Maximum $750,000, $1,000,000 Length of Coverage Choose between 6, 12, or 36 months. Benefts are limited to the Maximum Allowable Expense or each Covered Expense, in addition to any specifc limits stated in the policy. Benefts are limited to the Maximum Allowable Expense for each Covered Eligible Expense, in addition to any specifc limits stated in the policy. Organ and Tissue transplants Extended Care Facility up to $150 per day for a maximum of 30 days Inpatient prescription drugs Outpatient Surgical Facility Physical, Occupational, and Speech Therapy $50 per day and 20 visits combined Surgeon services in the hospital or outpatient surgical facility Note: this is a brief description of the plan benefts, which may vary by state. Be sure to check your policy carefully to make sure you are aware of any exclusions or limitations regarding coverage of preexisting conditions or health benefts (such as hospitalization, emergency services, maternity care, preventive care, prescription drugs, and mental health and substance use disorder services). Your policy might also have lifetime and/or annual dollar limits on health benefts. If this coverage expires or you lose eligibility for this coverage, you might have to wait until an open enrollment period to get other health insurance coverage. Financial Strength LifeShield plans are underwritten by the LifeShield National Insurance Co. Best is an independent global rating organization that examines insurance companies and publishes its opinion on their fnancial strength. With LifeShield, you and your family will fnd comfort in having fnancial protection from unforeseen medical expenses. This membership entitles doctors and hospital facilities who have contracted to provide specifc medical care at negotiated prices. Gallbladder Surgery for which a Covered Person received medical treatment, diagnosis, care or advice within the 60-month period 5. Treatment for Substance Abuse, unless specifcally produced any symptoms which would have caused a covered under the Policy as an Eligible Expense. Medications, vitamins, and mineral or food supplements this exclusion does not apply to a newborn child or newborn including pre-natal vitamins, or any over-the-counter adopted child who is added to coverage in accordance medicines, whether or not ordered by a Doctor. Any drug, treatment or procedure that either promotes or prevents conception including but not limited to: artifcial 2. Covered Persons will only be entitled to receive benefts sterilization or reversal of sterilization. Modifcations of the physical body in order to improve for Cancer that begins, by occurrence of symptoms or the psychological, mental or emotional well-being of the receipt of treatment more than 30 days following the Covered Person, such as sex-change surgery. Surgeries, treatments, services or supplies for cosmetic or aesthetic reasons, except for reconstructive surgery 3. Expenses during the frst 6 months after the Certifcate where expressly covered under the Policy. Total or partial hysterectomy, unless it is Medically Necessary due to diagnosis of carcinoma; 14. Dental treatment and dental surgery except as necessary involving the sinus; to restore or replace sound and natural teeth lost or. The benefts payable for the following conditions or under the Policy as an Eligible Expense. Charges for a Covered Dependent who is a newborn Psychiatric Association, and biofeedback and non-medical child not yet discharged from the Hospital, unless the self-care or self-help programs. Eyeglasses, contact lenses, hearing aids, hearing implants, sustained during or after birth. Care, treatment or supplies for the feet, orthopedic Complications of Pregnancy or if the life of the expectant shoes, orthopedic prescription devices to be attached mother would be at risk. Joint replacement or other treatment of joints, spine, treatment of corns, calluses or toenails. Care and treatment for hair loss including wigs, hair transplants or any drug that promises hair growth, 22. Surgeries, treatments, services or supplies which are whether or not prescribed by a Doctor. Telephone or Internet consultations and/or treatment or failure to keep a scheduled appointment. Treatment or diagnosis of allergies, except for emergency treatment of allergic reactions. Charges for travel or accommodations, except as expressly provided for local ambulance. Services received or supplies purchased outside the consequences of a non-covered treatment or condition. United States, its territories or possessions, or Canada, unless specifcally covered under the Policy as an Eligible 29. Services or supplies which are not included as Eligible Expenses as described herein. Biofeedback, acupuncture, recreational, sleep or mist including participating, instructing, demonstrating, therapy, holistic care of any nature, massage and guiding or accompanying others in the following: kinestherapy, excepted as provided for under Home operation of a fight in an aircraft other than a regularly Health Care. Hypnotherapy when used to treat conditions that are hot-air ballooning, hang-gliding, base jumping, mountain not recognized as Mental Disorders by the American climbing, bungee jumping, scuba diving, sail gliding, 8 Medical Expenses Not Covered (cont. Costs for Routine Physical Exams or other services not test of any motorized or non-motorized vehicle, rodeo needed for medical treatment, unless specifcally covered activities, or similar hazardous activities. Amounts in excess of the Usual and Customary charges made for covered services or supplies. Injuries or Sicknesses resulting from participation in interscholastic, intercollegiate or organized competitive 56. This does not include dependent children required to pay, or which would not have been billed, if participating in local community sports activities. Expenses to the extent that they are paid or payable wholly or partly to the effects of alcohol or drugs, other under other valid or collectible group insurance or medical than drugs taken in accordance with treatment prescribed prepayment plan. Charges that are eligible for payment by Medicare or any other government program except Medicaid. Expenses resulting from a declared or undeclared war, or from voluntary participation in a riot or insurrection. Expenses for which benefts are paid or payable under Exception does not apply to an act of terrorism. Upon written notice to Us of automobile insurance policy without regard to fault (does entry into such active duty, the unused premium will be not apply in any state where prohibited). It does not cover pre-existing conditions and you may be subject to the Affordable Care Act Shared Responsibility Tax. Feline Chronic Nasal Disease: Pathophysiologic Basis of Diagnosis and Therapy Stephan A. Normal nasal function is important in maintenance of olfactory function, but also plays a role in appetite and behavior in cats and dogs. Symptoms of nasal disease may be caused by any of a myriad of primary respiratory disorders or non-respiratory causes. Idiopathic chronic rhinitis is one of the most common chronic nasal disorders in dogs and cats. It is a diagnosis made by exclusion of other disorders, and usually requires chronic management. Other causes of chronic nasal symptoms include structural, mechanical, neoplastic, parasitic, infectious, and allergic disorders. The approach to chronic nasal disease should be designed to first identify or rule out primary nasal conditions with specific therapeutic options, then to secondarily manage chronic idiopathic inflammatory nasal conditions. Treatment of secondary infections and symptomatic therapy should be tertiary goals. The purpose of this session will be to review normal nasal structure and function, to use this information to highlight the potential effects of the loss of these functions, to provide the basis for a diagnostic and therapeutic approach to chronic nasal disease that can be largely accomplished without referral, and to provide insights into potential causes of treatment failure or relapses. The focus of these sessions will be on feline nasal disease, but many of these strategies will be applicable for canine chronic rhinitis as well. It is the primary site of entry for inhaled air in the feline respiratory system, and therefore has many important and diverse functions. The nasal cavity functions to efficiently filter, warm, and humidify inhaled air before it enters the more delicate distal tracheobronchial airways and alveolar parenchyma of the lung. In addition to olfactory sensory function, the nasal cavity also serves as a sensory organ for the detection of irritants and noxious inhaled substances. The goals of therapy for chronic rhinitis are largely aimed at restoring nasal function, so an understanding of normal nasal structure and function is essential to developing therapeutic strategies. Gross and Functional Anatomy of the Nose the feline nasal airway is divided into two passages by the nasal septum. The nasopharynx is defined as the airway posterior to the termination of the nasal septum and proximal to the termination of the soft palate. Inhaled air flows through the nostril openings, or nares, into the vestibule, which is a slight dilatation just inside the nares and before the main chamber of the nose. Unlike the more distal main nasal chamber that is surrounded by bone, the nasal vestibule is surrounded primarily by more flexible cartilage. The luminal surface is lined by a squamous epithelium similar to that of external skin. The rostral main chamber in cats has two turbinates, the maxilloturbinate (ventral nasal concha) and the nasoturbinate (dorsal nasal concha), that emanate medially from the lateral wall of the main chamber. The main chamber is divided by the maxilloturbinate and nasoturbinate into a dorsal, middle, and ventral meatus. These turbinates are lined by mucosa containing abundant capacitance vessels that are under autonomic control. Dilation of these vessels causes engorgement of the erectile mucosal tissue, leading to nasal congestion. In the caudal main chamber, the ethmoturbinates emanate rostrally from the dorsal septum and the ethmoid bone. These turbinates are primarily lined by olfactory epithelium, and contribute to the acute olfactory capacity of cats. Feline turbinates have complex folding and branching patterns that serve to increase nasal airway surface area for filtration, absorption, conditioning, and clearance. These turbinates also divide the nasal airspace into multiple narrow, tortuous columns that are vulnerable to obstruction. Nasal Breathing the upper airways provide the majority of the resistance in the respiratory tree (up to 75% of the inspiratory resistance). While cats are technically capable oronasal breathers, many cats will maintain nasal breathing, even in the face of severe nasal obstruction or cardiopulmonary dysfunction. A switch to oral breathing in a cat usually suggests that there is a significant reduction in cardiopulmonary reserve. It is therefore very important that nasal airway patency be preserved in cats presenting with any type of respiratory dysfunction. After passing through the nasal vestibule, inhaled air courses through the narrowest part of the entire respiratory tract, the nasal valve (ostium internum), into the main nasal chamber. All nasally inspired air passes through the main chamber into the nasopharyngeal meatus prior to passage through the laryngopharynx into the lower airways. The cross sectional area of the nasal airways decreases by 4-5x between the main chamber and the nasopharynx, requiring an increase in flow rate to accommodate bulk flow. Because of this abrupt change in airway caliber at this site, even minor changes in the diameter of the nasopharyngeal airway lumen can have profound effects on inspiratory airflow and respiratory effort. Nasal Filtration and Mucociliary Clearance Most of the luminal surfaces of the nasal mucosa (with the exception of the most proximal regions of the nasal vestibule) are covered by mucus.
Buy super p-force oral jelly paypal. treatment in acupuncture - ஆன்மை குறைவு .. Dr. B. Hariharan - male impotence :infertility.