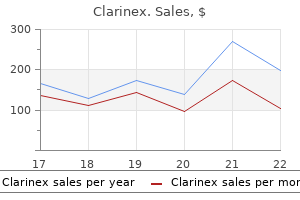
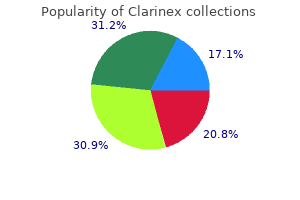
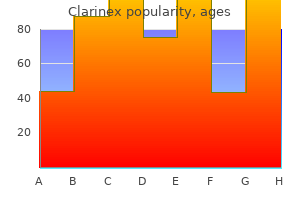
Clarinex
Eddie Hooker, M.D.
- Assistant Professor
- University of Louisville
- Louisville, KY
If intakes of fat allergy symptoms to condoms cheap clarinex 5mg without a prescription, along with carbohydrate and protein allergy symptoms pet dander buy 5 mg clarinex with visa, are inadequate to meet energy needs allergy forecast davis ca purchase clarinex 5 mg free shipping, the individual will be in negative energy balance allergy shots benefits buy generic clarinex on line. Depending on the severity and duration allergy testing portland oregon best order clarinex, this may lead to malnutrition or starvation allergy symptoms goose down order clarinex 5 mg fast delivery. In some populations, fat intakes are very low and body weight and health are maintained by high intakes of carbohydrate (Bunker et al. Clearly, humans have the ability to adapt metabolically to a wide spectrum of fat-to-carbohydrate intake ratios. In the short term, an isocaloric diet can be either very high or very low in fat with no obvious differences in health. The critical question therefore is, Are there optimal fat-to-carbohydrate ratios for longterm health, and if so, what are they One potential concern over fat restriction is the potential for reduction in total energy intake, which is of particular relevance for infants and children, as well as during pregnancy when there is a relatively high energy requirement for both energy expenditure and for fetal development. These changes include a reduction in high density lipoprotein cholesterol concentration, an increase in serum triacylglycerol concentration, and higher responses in postprandial glucose and insulin concentrations. In fact, some populations that consume low fat diets and in which habitual energy intake is relatively high have a low prevalence of these chronic diseases (Falase et al. Conversely, in sedentary populations, such as that of the United States where overweight and obesity are common, high carbohydrate, low fat diets induce changes in lipoprotein and glucose/insulin metabolism in ways that could raise risk for chronic diseases (see Chapter 11). Available prospective studies have not concluded whether low fat, high carbohydrate diets provide a health risk in the North American population. Chronic nonspecific diarrhea in children has been suggested as a potential adverse effect of low fat diets. It is considered a disorder of intestinal motility that may improve with an increase in dietary fat intake in order to slow gastric emptying and alter intestinal motility (Cohen et al. Detailed discussion on fat intake and risk of chronic disease is provided in Chapter 11. Because adipose tissue lipids in free-living, healthy adults contain about 10 percent of total fatty acids as linoleic acid, biochemical and clinical signs of essential fatty acid deficiency do not appear during dietary fat restriction or malabsorption when they are accompanied by an energy deficit. In this situation, release of linoleic acid and small amounts of arachidonic acid from adipose tissue reserves may prevent development of essential fatty acid deficiency. However, during parenteral nutrition with dextrose solutions, insulin concentrations are high and mobilization of adipose tissue is prevented, resulting in development of the characteristic signs of essential fatty acid deficiency. Studies on patients given fat-free parenteral feeding have provided great insight into defining levels at which essential fatty acid deficiency may occur. When dietary essential fatty acid intake is inadequate or absorption is impaired, tissue concentrations of arachidonic acid decrease, inhibition of the desaturation of oleic acid is reduced, and synthesis of eicosatrienoic acid from oleic acid increases. The characteristic signs of deficiency attributed to the n-6 fatty acids are scaly skin rash, increased transepidermal water loss, reduced growth, and elevation of the plasma ratio of eicosatrienoic acid:arachidonic acid (20:3n-9:20:4n-6) to values greater than 0. In addition to the clinical signs mentioned above, essential fatty acid deficiency in special populations has been linked to hematologic disturbances and diminished immune response (Bistrian et al. Thus, the amount of n-3 fatty acids and their effects on arachidonic acid metabolism are relevant to many chronic diseases. Studies in rodents and nonhuman primates have consistently demonstrated that prolonged feeding with diets containing very low amounts of linolenic acid result in reductions of visual acuity thresholds and electroretinogram A and B wave recordings, which were prevented when linolenic acid was included in the diet (Anderson et al. A variety of changes in learning behaviors in animals fed linolenic aciddeficient diets have also been reported (Innis, 1991). The compensatory increase in 22 carbon chain n-6 fatty acids results in maintenance of the total amount of n-6 and n-3 polyunsaturated fatty acids in neural tissue. For example, rates of oxidation of linolenic acid are much higher than for linoleic acid (Clouet et al. Unlike essential fatty acid deficiency (n-6 and n-3 fatty acids), plasma eicosatrienoic acid (20:3n-9) remains within normal ranges and skin atrophy and scaly dermatitis are absent when the diet is deficient in only n-3 fatty acids. Currently, there are no accepted plasma n-3 fatty acid or n-3 fatty acid-derived eicosanoid concentrations for indicating impaired neural function or impaired health endpoints. These studies showed no effect of the level of dietary fat on growth when energy intake is adequate. Fat Balance (Maintenance of Body Weight) Because fat is an important source of energy, studies have been conducted to ascertain whether dietary fat influences energy expenditure and the amount of fat needed in the diet to achieve fat balance and therefore maintain body weight. These studies demonstrated that the amount of fat in the diet does not affect energy expenditure and thus the amount of energy required to maintain body weight (Hill et al. Saturated Fatty Acids Saturated fatty acids are a potential fuel source for the body. In addition, they are important structural fatty acids for cell membranes and other functions and therefore are essential for body functions. These fatty acids, however, can be synthesized as needed for these functions from other fuel sources and have not been associated with any beneficial role in preventing chronic disease. Nevertheless, monounsaturated fatty acids can be biosynthesized from other fuel sources and therefore are not essential in the diet. Early signs of essential fatty acid deficiency include rough and scaly skin, which if left untreated, develops into dermatitis (Jeppesen et al. In studies of patients with dermatitis who were receiving parenteral nutrition, the ratio of eicosatrienoic acid:arachidonic acid (20:3n-9:20:4n-6) in plasma was elevated. As described earlier, when present in adequate amounts, linoleic acid is converted to arachidonic acid through a multi-step process involving 6 and 5 desaturases (see Figure 8-1); however, in the absence of linoleic acid, 6 and 5 desaturases convert oleic acid to eicosatrienoic acid. The increase in eicosatrienoic acid concentration, which occurs in the absence of n-6 fatty acids or the combined absence of n-6 and n-3 fatty acids, led Holman (1960) to define a plasma triene:tetraene ratio of greater than 0. Optimal plasma or tissue lipid concentrations of linoleic acid, arachidonic acid, and other n-6 fatty acids or the ratios of certain n-6:n-3 fatty acids have not been established. Because the n-6 fatty acid intake is generally well above the levels needed to maintain a triene:tetraene ratio below 0. In these studies, after developing an essential fatty acid deficiency, patients were treated with linoleic acid. These studies observed symptoms such as rash, scaly skin, and ectopic dermititis; reduced serum tetraene concentrations, increased serum triene concentration; and a triene:tetraene ratio greater than 0. Sensory neuropathy and visual problems in a young girl given parenteral nutrition with an intravenous lipid emulsion containing only a small amount of linolenic acid were corrected when the emulsion was changed to one containing generous amounts of linolenic acid (Holman et al. Nine patients with an n-3 fatty acid deficiency had scaly and hemorrhagic dermatitis, hemorrhagic folliculitis of the scalp, impaired wound healing, and growth retardation (Bjerve, 1989). The possibility of other nutrient deficiencies, such as vitamin E and selenium, has been raised (Anderson and Connor, 1989; Meng, 1983). A series of papers have described low tissue n-3 fatty acid concentrations in nursing home patients fed by gastric tube for several years with a powdered diet formulation that provided about 0. Skin lesions were resolved following supplementation with cod liver oil and soybean oil or ethyl linolenate (Bjerve et al. Concurrent deficiency of both n-6 and n-3 fatty acids in these patients, as in studies of patients supported by lipid-free parenteral nutrition, limits interpretation of the specific problems caused by inadequate intakes of n-3 fatty acids. In these tissues, the phospholipid sn-1 chain is usually a saturated fatty acid. Reduced growth or changes in food intake have not been noted in the extensive number of studies in animals, including nonhuman primates fed for extended periods on otherwise adequate diets lacking n-3 fatty acids. Thus, the dietary n-3 fatty acid requirement involves the activity of the desaturase enzymes and factors that influence the desaturation of linolenic acid in addition to the amount of the n-3 fatty acid. Activity of 6 and 5 desaturases has been demonstrated in human fetal tissue from as early as 17 to 18 weeks of gestation (Chambaz et al. Furthermore, the ability to convert linolenic acid appears to be greater in premature infants than in older term infants (Uauy et al. Some have included arachidonic acid or linolenic acid (18:3n-6), the 6 desaturase product of linoleic acid. These include a prospective, double-blind design with a sufficient number of infants randomized to control for the multiple genetic, environmental, and dietary factors that influence infant development and to detect meaningful treatment effects (Gore, 1999; Morley, 1998); the amount and balance of linoleic and linolenic acid; the duration of supplementation; the age at testing and tests used; and the physiological significance of any statistical differences found. Early studies by Makrides and colleagues (1995) reported better visual evoked potential acuity in infants fed formula with 0. However, this group did not confirm this finding in subsequent studies with formulas containing 0. The effect of low n-6:n-3 ratios (high n-3 fatty acids) on arachidonic acid metabolism is also of concern in growing infants. Additionally, no differences in growth were found among infants fed formulas with 1. In conclusion, randomized clinical studies on growth or neural development with term infants fed formulas currently yield conflicting results on the requirements for n-3 fatty acids in young infants, but do raise concern over supplementation with long-chain n-3 fatty acids without arachidonic acid. Trans Fatty Acids and Conjugated Linoleic Acid Small amounts of trans fatty acids and conjugated linoleic acid are present in all diets. However, there are no known requirements for trans fatty acids and conjugated linoleic acid for specific body functions. Pancreatic secretion after initial stimulation with either secretin or pancreozymin is not diminished with age (Bartos and Groh, 1969). The ratio of mean surface area to volume of jejunal mucosa has been reported not to differ between young and old individuals (Corazza et al. Total gastrointestinal transit time appears to be similar between young and elderly individuals (Brauer et al. Documented changes with age may be confounded by the inclusion of a subgroup with clinical disorders. The presence of bile salt-splitting bacteria normally present in the small intestine of humans is of potential significance to fat absorption. In addition, increases in fat malabsorption have not been demonstrated in normal elderly compared to younger individuals (Russell, 1992). Exercise Imposed physical activity decreased the magnitude of weight gain in nonobese volunteers given access to high fat diets (60 percent of energy) (Murgatroyd et al. Thus, high fat diets may cause positive fat balance, and therefore weight gain, only under sedentary conditions. These results are consistent with epidemiological evidence that show interactions between dietary fat, physical activity, and weight gain (Sherwood et al. Higher total fat diets can probably be consumed safely by active individuals while maintaining body weight. Although in longitudinal studies of weight gain, where dietary fat predicts weight gain independent of physical activity, it is important to note that physical activity may account for a greater percentage of the variance in weight gain than does dietary fat (Hill et al. High fat diets (69 percent of energy) do not appear to compromise endurance in trained athletes (Goedecke et al. This effect on training was not observed following long-term adaptation of high fat diets. Genetic Factors Studies of the general population may underestimate the importance of dietary fat in the development of obesity in subsets of individuals. Some data indicate that genetic predisposition may modify the relationship between diet and obesity (Heitmann et al. Additionally, some individuals with relatively high metabolic rates appear to be able to consume high fat diets (44 percent of energy) without obesity (Cooling and Blundell, 1998). Intervention studies have shown that those individuals susceptible to weight gain and obesity appear to have an impaired ability to increase fat oxidation when challenged with high fat meals and diets (Astrup et al. Animal studies show that there are important gene and dietary fat interactions that influence the tendency to gain excessive weight on a high fat diet (West and York, 1998). The formation of nicotinamide adenine dinucleotide, resulting from ethanol oxidation, serves as a cofactor for fatty acid biosynthesis (Eisenstein, 1982). Similar to carbohydrate, alcohol consumption creates a shift in postprandial substrate utilization to reduce the oxidation of fatty acids (Schutz, 2000). Significant intake of alcohol (23 percent of energy) can depress fatty acid oxidation to a level equivalent to storing as much as 74 percent as fat (Murgatroyd et al. If the energy derived from alcohol is not utilized, the excess is stored as fat (Suter et al. Interaction of n-6 and n-3 Fatty Acid Metabolism the n-6 and n-3 unsaturated fatty acids are believed to be desaturated and elongated using the same series of desaturase and elongase enzymes (see Figure 8-1). In vitro, the 6 desaturase shows clear substrate preference in the following order: linolenic acid > linoleic acid > oleic acid (Brenner, 1974). It is not known if these are the 6 desaturases that are responsible for metabolism of linoleic acid and linolenic acid or a different enzyme (Cho et al. An inappropriate ratio may involve too high an intake of either linoleic acid or linolenic acid, too little of one fatty acid, or a combination leading to an imbalance between the two series. The provision of preformed carbon chain n-6 and n-3 fatty acids results in rapid incorporation into tissue lipids. Arachidonic acid is important for normal growth in rats (Mohrhauer and Holman, 1963). Later in life, risk of certain diseases may be altered by arachidonic acid and arachidonic acid-derived eicosanoids. Consequently, the desirable range of n-6:n-3 fatty acids may differ with life stage. Similarly, stable isotope studies have shown that increased intakes of linolenic acid result in decreased conversion of linoleic acid to its metabolites, and the amounts metabolized to longerchain metabolites is inversely related to the amount oxidized (Vermunt et al. These eicosanoids have been shown to have beneficial and adverse effects in the onset of platelet aggregation, hemodynamics, and coronary vascular tone. More recent, large clinical trials with infants fed formulas providing linoleic acid: linolenic acid ratios of 5:1 to 10:1 found no evidence of reduced growth or other problems that could be attributed to decreased arachidonic acid concentrations (Auestad et al. Clark and coworkers (1992) concluded that intake ratios less than 4:1 were likely to result in fatty acid profiles markedly different from those from infants fed human milk.
However allergy medicine ok while breastfeeding order discount clarinex, many common age-related changes do predispose elderly patients to incontinence allergy medicine like allegra d order clarinex visa. It is important to remember that these changes are found in many healthy allergy medicine birth control cheap 5 mg clarinex otc, continent elderly persons allergy medicine isn't working buy clarinex us. Elderly patients excrete a larger percentage of fluid late in the day (increasing nocturia) allergy immunotherapy buy 5mg clarinex, and urogenital atrophy leads to decreased internal urethral sphincter sensitivity allergy medicine for 18 month old cheap clarinex 5mg with amex. Diuretics also may cause secondary incontinence, and may need to be avoided unless necessary. Stool impaction is thought to be a causative factor in up to 10% of patients with incontinence, and disimpaction may restore continence. Atrophic vaginitis may also be causative, and treatment may improve the situation. Due to detrusor hyperactivity, patients often complain of a strong urge followed by an involuntary loss of urine. Functional incontinence refers to a limitation that does not allow the patient to void in the bathroom (bed rest, paralysis, severe dementia) and does not generally relate to the urinary tract. Stress incontinence is the loss of urine associated with increased abdominal pressure, and overflow incontinence is incontinence due to overdistention of the bladder. Patients complain of involuntary loss of urine associated with increases in intra-abdominal pressure (when sneezing, coughing, laughing, or exercising). Functional incontinence refers to a limitation that 174 Family Medicine does not allow the patient to void in the bathroom (bed rest, paralysis, severe dementia) and does not generally relate to the urinary tract. Urge incontinence is the loss of urine following a strong urge, and overflow incontinence is incontinence due to overdistention of the bladder. Incontinence is usually a frequent or constant leakage of small amount, but occasionally a large amount of urine is lost without warning. Functional incontinence refers to a limitation that does not allow the patient to void in the bathroom (bed rest, paralysis, severe dementia) and does not generally relate to the urinary tract. Stress incontinence is the loss of urine associated with increased abdominal pressure, and urge incontinence is preceded by a strong urge to urinate. A postvoid residual greater than 200 mL indicates inadequate bladder emptying and is consistent with overflow incontinence. Patients are asked to squeeze the muscles in the genital area as if they were trying to stop the flow of urine from the urethra. Patients are then taught to contract these muscles and hold them during situations where incontinence may occur. They are most useful to treat stress incontinence, but may help with mixed incontinence as well. For urge incontinence, anticholinergic medications are the drugs of choice with oxybutynin (Ditropan) and tolterodine (Detrol) both indicated for symptoms. Pseudoephedrine has been shown to help stress incontinence, Acute Complaints Answers 175 trimethoprim-sulfamethoxazole has been shown to help in the case of prostatitis, and finasteride and terazosin will help frequent voiding caused by prostatic hyperplasia. Gonadal dysgenesis is the most common cause of primary amenorrhea, responsible for about 50% of the cases. Constitutional delay of puberty, although common in boys, is an uncommon cause of amenorrhea in girls, but clinically is very hard to distinguish from other more common causes. Polycyctic ovarian syndrome is common, and is responsible for about 30% of the cases of secondary amenorrhea. It is characterized by androgen excess, and symptoms include irregular or absent menses, hirsuitism, acne, and virilization. Functional hypothalamic amenorrhea is usually a result of anorexia, rapid weight loss, rigorous exercise, or significant emotional stress. Hypothyroidism and hyperprolactinemia can both be associated with secondary amenorrhea, but are less common causes. Since these patients do not ovulate, progesterone from the corpus luteum is not secreted, the withdrawal from which would normally cause endometrial sloughing. It is the most common cause of dysfunctional uterine bleeding in women younger than 20 years of age, accounting for about 95% of cases. When women are within 2 years of menarche, this is 176 Family Medicine especially common, and can be followed expectantly. Ovulatory bleeding due to fluctuations in estrogen and progesterone levels is also a cause of abnormal bleeding, but accounts for only about 10% of cases. In fact, this is usually the first step in the evaluation of this problem, after performing the examination and ruling out sexually transmitted infections or anatomic abnormalities. Ultrasound evaluation may be needed, but this would not be the next step in the evaluation of this condition. This can occur either by using medications that inhibit prostaglandin synthesis, or by suppressing ovulation. While opiate use may help with pain control, it does not inhibit prostaglandin synthesis and may lead to addiction. When hyperprolactinemia is related to medication, the measured prolactin level is usually less than 100 ng/mL. Neurologic drugs that can increase prolactin levels include Acute Complaints Answers 177 sumatriptan, valproate, and ergot derivatives. Estrogens and contraceptives can also elevate prolactin, as can some cardiovascular drugs (atenolol, verapamil, reserpine, and methyldopa). Any bleeding in the week after the administration of Provera indicates that the patient has sufficient estrogen to menstruate, and that the amenorrhea is likely due to anovulation. When there is no withdrawal bleeding, it either indicates inadequate estrogen production or an outflow tract obstruction. No withdrawal bleeding after an estrogen-progestin challenge indicates an outflow tract obstruction or an anatomic defect. In general, if the history and physical examination are normal, no further workup is necessary, and a trial of treatment is indicated. Gonorrhea and Chlamydia cultures may be necessary in the initial evaluation, but if the history and examination are not suggestive of infection, cultures are not necessary. Ultrasound, hysterosalpingography, and laparoscopy are not indicated at this stage of the evaluation. Pain from endometriosis usually begins several days before menses and may last 178 Family Medicine throughout the entire cycle. When symptoms are present, it is usually described as pelvic pressure, bloating menorrhagia or metorrhagia, depending on the tumor size or location. Disorientation is characteristic of both processes, as is a disturbed sleep-wake cycle. His history of hypertension would lead one to think of multi-infarct dementia, rather than delirium. Responsiveness to questions may be a feature of either process, though patients with delirium often have a shortened attention span. The abrupt onset of a mental status change is consistent with delirium as opposed to dementia, which occurs insidiously. With his severe hypertension, a stroke may be considered, but unlikely without focal neurological deficits. Pinpoint pupils would be more consistent with narcotic excess, unlikely given his vital signs and history. Dilated pupils suggests sympathetic outflow, and may be consistent with delirium tremens, but the history and physical is not consistent with this. Anisocoria of 1 mm is a nonspecific finding that can be seen in normal individuals. Fluoxetine usually does not cause a withdrawal syndrome, but may be associated with depressive symptoms. The inability to complete serial sevens (count backwards from 100 by 7s) may be related to educational level. Although her symptoms have appeared recently, it is often difficult to pinpoint the exact onset of dementia. Metoclopramide can improve gastric motility and help her symptoms more than the other antiemetics listed. In this case, mild pain, followed by the acute onset of distension, nausea, and vomiting is consistent with ileus or obstruction. Hyperactive bowel sounds lead one to think of obstruction; with an ileus bowel sounds are absent. Gastroenteritis begins acutely, but is usually not preceded by mild abdominal pain. Diverticulosis and diverticulitis would cause pain, but would be less likely to present with nausea, vomiting, and distension. It is usually seen during times of social stress or in patients with a past history of a psychiatric disorder. While young girls in this age group are at risk for anorexia and bulimia, sufferers usually do not seek medical attention or treatment until concerned others bring the condition to medical attention. A central nervous system malignancy is possible, if the lesion involves the vomiting center, but one would expect to see nutritional deficit in this case. Symptoms typically begin acutely and are associated with typical viral syndrome symptoms. Oral rehydration is indicated as long as there are no signs of 180 Family Medicine severe dehydration. Intravenous rehydration and antiemetics may have a role, but only in more severe cases. While the laboratory findings in acute pancreatitis are often nonspecific, elevated serum amylase in the right clinical setting is often suggestive. In establishing a cause for pancreatitis, history is key, but some laboratory findings are helpful. When nausea happens before eating in the morning, likely etiologies include pregnancy, uremia, alcohol withdrawal, and increased intracranial pressure (meningitis or space-occupying lesions). Cholelithiasis is associated with nausea, vomiting, and pain after eating fatty foods. Vestibular disorders cause nausea without any clear association with meals or time of day. Nausea associated with cholelithiasis is associated with pain, usually after eating fatty foods. Vestibular disorders cause nausea without clear relationship to eating, and a brain tumor would cause morning symptoms. Reflux may be possible, but is less likely to be associated with weight loss and dehydration. Intussesception is associated with significant abdominal pain, and hemoccult positive stools. Small bowel obstructions are less likely, and are associated with high-pitched bowel sounds. The diagnostic test of choice would be a right upper quadrant ultrasound to identify stones in the gallbladder. Amylase and lipase may be positive if the patient develops secondary pancreatitis, but are unlikely to be elevated until that point. Hemoccult testing, abdominal x-rays, and upper endoscopy are all likely to be normal. The phenothiazines (Compazine and Phenergan) generally cause drowsiness, dry mouth, and dizziness. Zofran is a serotonin receptor antagonist, and may cause dizziness and headache. Reglan is a prokinetic agent, and can cause diarrhea and extrapyramidal reactions. Family history of similar symptoms would not be a risk factor for cardiac disease. While hyperthyroidism may cause atrial fibrillation, the patient would likely have other additional symptoms. Stimulant abuse would likely cause sinus tachycardia, and while hyperthyroidism can cause premature beats, the patient would likely experience other symptoms. Consultation with an electrophysiologist may be appropriate, depending on the results of the testing. Treatment usually consists of radiofrequency ablation, but pharmacologic therapy is also an option. On physical examination, the examiner feels a smooth mobile adnexal mass with peritoneal signs if the cyst ruptures. Ectopic pregnancy may present with similar symptoms, but menses would not be normal. Uterine leiomyoma would be associated with an enlarged uterus, and appendicitis would be associated with nausea and anorexia. Fever, vaginal discharge, dysuria, and occasionally abnormal vaginal bleeding may be associated symptoms.
Human lesions show a decrease in the number of virus particles as the disease progresses allergy symptoms medication buy clarinex 5mg on line. Preventive measures: Good personal hygiene and washing the exposed area with soap and water allergy medicine non drowsy effective clarinex 5mg. The efcacy and safety of Parapoxvirus vaccines in animals has not been fully determined allergy testing for gluten order on line clarinex. Control of patient allergy dizziness order clarinex with amex, contacts and the immediate environment: 1) Report to local health authority: Not required allergy forecast rochester mn order 5 mg clarinex with mastercard, but desirable when a human case occurs in areas not previously known to have the infection allergy medicine makes me tired proven clarinex 5 mg, Class 5 (see Reporting). In disseminated cases all viscera may be affected; adrenal glands are especially susceptible. The less common juvenile (acute) form is characterized by reticuloendothelial system involvement and bone marrow dysfunction. Keloidal blastomycosis (Lobo disease), a disease involving skin only, formerly confused with paracoccidioidomycosis, is caused by Lacazia loboi, a fungus known only in tissue form and not yet grown in culture. Workers in contact with soil, such as farmers, laborers, and construction workers are especially at risk. X-ray ndings may include diffuse and/or segmental inltrates, nodules, cavities, ring cysts and/or pleural effusions. The sputum generally contains orange-brown ecks, sometimes diffusely distributed, in which masses of eggs are seen microscopically and establish the diagnosis. However, acid-fast staining for tuberculosis destroys the eggs and precludes diagnosis. Eggs are also swallowed, especially by children, and may be found in feces by some concentration techniques. The disease has been quasi-eliminated from Japan, while fewer than 1000 people are infected in the Republic of Korea. Of the Latin American countries, Ecuador is the most affected, with about 500 000 estimated infections; cases have also occurred in Brazil, Colombia, Costa Rica, Mexico, Peru and Venezuela. Larvae excyst in the duodenum, penetrate the intestinal wall, migrate through the tissues, become encapsulated (usually in the lungs) and develop into egg-producing adults. Larvae (cercariae) emerge from the snails to encyst in freshwater crabs and craysh. Pickling of these crustaceans in wine, brine or vinegar, a common practice in Asia, does not kill encysted larvae. The long, variable, poorly dened interval until symptoms appear depends on the organ invaded and the number of worms involved. Preventive measures: 1) Educate the public in endemic areas about the life cycle of the parasite. Control of patient, contacts and the immediate environment: 1) Report to local health authority: Ofcial report not ordinarily justiable, Class 5 (see Reporting). Epidemic measures: In an endemic area, the occurrence of small clusters of cases, or even sporadic infections, is an important signal for examination of local waters for infected snails, crabs and craysh, and determination of reservoir mammalian hosts, to establish appropriate controls. Crab lice (Phthirus pubis) usually infest the pubic area; more rarely facial hair (including eyelashes in heavy infestations), axillae and body surfaces. Lice are host-specic and those of lower animals do not infest humans, although they may be present transiently. The body louse is the species involved in outbreaks of epidemic typhus caused by Rickettsia prowazeki, trench fever caused by R. Outbreaks of head lice are common among children in schools and institutions everywhere. Body lice are prevalent among populations with poor personal hygiene, especially in cold climates where heavy clothing is worn and bathing is infrequent or when people cannot change clothes. Lice leave a febrile host; fever and overcrowding increase transfer from person to person. The average life cycle of the body or head louse extends over a period of 18 days; that of the crab louse, 15 days. Control of patient, contacts and the immediate environment: 1) Report to local health authority: Ofcial report not ordinarily justiable; school authorities should be informed, Class 5 (see Reporting). Lindane and benzyl benzoate are no longer recommended or registered because of toxicity, side-effects and low efcacy. For body lice: Clothing and bedding should be washed using the hot water cycle of an automatic washing machine or dusted with pediculicides using power dusters, hand dusters or 2-ounce sifter cans. Epidemic measures: Mass treatment as recommended in 9B7 above, using insecticides clearly known to be effective against prevalent strains of lice. In typhus epidemics, individuals may protect themselves by wearing silk or plastic clothing tightly fastened around wrists, ankles and neck, and by impregnating their clothes with repellents or permethrin. Disaster implications: Diseases for which body and head lice are vectors are particularly prone to occur at times of social upheaval (see Typhus fever, section I, Epidemic louse-borne). Paroxysms are characterized by repeated violent cough; each series of paroxysms has many coughs without intervening inhalation and can be followed by a characteristic crowing or high-pitched inspiratory whoop. Paroxysms frequently end with the expulsion of clear, tenacious mucus, often followed by vomiting. Infants under 6 months, vaccinated children, adolescents and adults often do not have the typical whoop or cough paroxysm. The vast majority of deaths occur in infants under 6 months, often in those too young to have completed primary immunization. In recent years, all deaths from pertussis in most industrialized countries occurred in infants under 6 months. In nonimmunized populations, especially those with underlying malnutrition and multiple enteric and respiratory infections, pertussis is among the most lethal diseases of infants and young children. Complications include pneumonia, atelectasia, seizures, encephalopathy, weight loss, hernias and death. Pneumonia is the most common cause of death; fatal encephalopathy, probably hypoxic, and inanition from repeated vomiting occasionally occur. Case-fatality rates in unprotected children are less than 1 per thousand in industrialized countries; in developing countries they are estimated at 3. In several industrialized countries with high rates of infant immunization for many years an increasing proportion of cases has been reported in adolescents and adults, whose symptoms varied from a mild, atypical respiratory illness to the full-blown syndrome. Many such cases occur in previously immunized persons and suggest waning immunity following immunization. Parapertussis is a similar but occasional and milder disease due to Bordetella parapertussis. Diagnosis is based on the recovery of the causal organism from nasopharyngeal specimens obtained during the catarrhal and early paroxysmal stages on appropriate culture media. Indirect diagnosis (serology) consists of detecting specic antibodies in the serum of infected individual, collected at the beginning of cough (acute serum) and on serum collected one month later (convalescent serum). The presence of high level of antibodies in the serum of a non-vaccinated individual indicates infection. Serology cannot be used for diagnosis during the year following vaccination since it does not differentiate between antibodies due to the vaccine or to natural infection Differentiation between B. A marked decline has occurred in incidence and mortality rates during the past 40 years, chiey in communities with active immunization programs and where good nutrition and medical care are available. In 1999, despite a global vaccination coverage of around 80%, there were still an estimated 48. Incidence rates have increased in countries where pertussis immunization rates fell in the past. Japan in the early 1980s, Sweden and the United Kingdom), and rose again when immunization programs were reestablished. In countries with high vaccination coverage, the incidence rate in children under 15 is less than 1 per 100 000. In vaccinated populations, bacteria are frequently brought home by an older sibling and sometimes by a parent. Thereafter, communicability gradually decreases and becomes negligible in about 3 weeks, despite persisting spasmodic cough with whoop. When treated with erythromycin, clarithromycin or azithromycin, patients are no longer contagious after 5 days of treatment. Incidence is highest in children under 5 years except where infant vaccination programs have been very effective and a shift has occurred toward adolescents. One attack usually confers prolonged immunity, although subsequent attacks (some of which may be attributable to B. Cases in previously immunized adolescents and adults in countries with long-standing and successful immunization programs occur because of waning immunity and are a source of infection for non immunized young children. Preventive measures: 1) Immunization is the most rational approach to pertussis control; and whole-cell vaccine against pertussis (wP) has been effective in preventing pertussis for more than 40 years. Educate the public, particularly parents of infants, about the dangers of whooping cough and the advantages of initiating immunization on time (between 6 weeks and 3 months depending on the country) and adhering to the immunization schedule. This continues to be important because of the wide negative publicity given to adverse reactions. In terms of severe adverse effects aP and wP vaccines appear to have the same high level of safety; reactions (local and transient systemic) are less commonly associated with aP vaccines. Similar high efcacy levels (more than 80%) occur with the best aP and wP vaccines although the level of efcacy may vary within each group. Protection is greater against severe disease and begins to wane after about 5 years. Although the use of aP vaccines is less commonly associated with local and systemic reactions such as fever, price considerations affect their use and wP vaccines are the vaccines of choice for most developing countries. In countries where immunization programs have considerably reduced pertussis incidence, a booster dose approximately one year after the primary series is warranted. Vaccines containing wP are not recommended after the seventh birthday since local reactions may be increased in older children and adults. Formulations of acellular pertussis vaccine for use in adolescents and adults have been licensed and are available in several countries. Prolonged crying and febrile seizures are less common (1 in 100); hypotonic-hyporesponsive episodes are rare (1 in 2000). The only true contraindication to immunization with aP or wP is an anaphylactic reaction to a previous dose or to any constituent of the vaccine. In young infants with suspected evolving and progressive neurological disease, immunization may be delayed for some months to permit diagnosis in order to avoid possible confusion about the cause of symptoms. Clarithromycin and azithromycin are expensive but better tolerated alternatives.
If there is no recurrence without medication in four years allergy symptoms in mouth clarinex 5mg without a prescription, the risk may then become acceptable for medical certification allergy symptoms swollen lips cheap clarinex 5 mg otc. Consideration should not be given until a four-year seizure-free and medication-free observation period has been achieved allergy symptoms plus fever order clarinex 5mg on line. With normal studies and no risk factors allergy medicine for dogs buy discount clarinex 5 mg on line, recurrence risk after four years approximates that of the normal population allergy symptoms early pregnancy order 5mg clarinex overnight delivery. Embolic stroke (artery to artery or cardio-embolic source) must also be considered allergy symptoms wine generic clarinex 5mg without a prescription. In the young, additional factors must be considered such as hypercoaguable states, patent foramen ovale, and arteriopathies. Clearly the existence of any persistent neurological deficit must be addressed in terms of functional compromise. Beyond the first year, recurrence risk is about four per cent per year, with some variability depending on stroke subtype. Medical certification is appropriate when cause and risk factors have been identified and addressed and a recurrence risk has been assessed. Recurrent stroke may cause sudden incapacitation, and a recurrence risk exceeding one per cent per year is not acceptable. A recurrence-free observation period is appropriate prior to medical certification following ischaemic stroke, and this will vary dependent upon mechanism and risk factors. If an individual with arterial dissection has no recurrence in one year, risk recurrence thereafter is less than one per cent per year. Vascular malformations including cavernous angiomas may also lead to intracerebral bleeding, sometimes with complete recovery. Though surgical cure of a vascular malformation might preclude re-bleeding, the risk of residual seizures may still bar certification. There are exceptions in which tissue destruction is minimal and recovery is complete or near complete. A oneto two-year observation period is appropriate following haemorrhagic stroke. A full neurological evaluation indicating satisfactory recovery and freedom from relevant risk factors may allow medical certification at that time. Aneurysms ordinarily arise from major arteries at the base of the brain (Circle of Willis) and are thought to develop from congenital changes in the muscular wall of the artery and degenerative changes in the internal elastic lamina. Death occurs in 23 per cent, and half of the survivors have significant disability. Sequelae may include focal neurological deficit, seizures, and cognitive impairment. Absent these conditions and with a period of symptom-free observation, medical certification may be possible. If there is no recurrence within one year, statistics reveal an acceptably low risk of recurrence thereafter. In another specific condition, called peri-mesencephalic or pre-pontine subarachnoid haemorrhage, recurrence risk is low. Partial obliteration of an aneurysm with residual lumen may present an unacceptable risk. For subarachnoid haemorrhage of unknown cause, a one-year observation period is also warranted. The presence of a vascular malformation (cavernous angioma, arteriovenous malformation) requires individual evaluation. Residual malformation, haemosiderin deposition and other factors will affect risk for recurrent haemorrhage or seizure, and medical certification may not be possible. Most head injuries, including some with a linear skull fracture, do not involve brain injury. Liberal use of modern imaging techniques may indicate parenchymal injury (localized haemorrhage) in individuals with no clinical signs or symptoms of injury. It is important to determine the nature and severity of injury as part of the evaluation. Symptomatic medications are often employed, precluding medical certification until the condition subsides. Medical records and current neurological functioning will provide information regarding persistent deficit. When indicated, detailed neuropsychological testing by a qualified examiner may document the presence or absence of any cognitive residual sequelae. With penetrating injuries involving violation of the cranial vault, the risk is high and may approach 40 per cent. In more commonly occurring closed head injuries, risk is a much lower five per cent. Cerebral contusion, parenchymal haematoma, post-traumatic amnesia beyond one day, depressed skull fracture and subdural haematoma confer increased risk. With penetrating injuries, 97 per cent of the risk will have been achieved in three years, though some elevated risk still persists ten years after the injury. Depending upon severity, focal neurological deficit may warrant a six months to two years period of observation for maximal neurological recovery. In individuals with neuropsychological residual changes, usually indicating significant traumatic brain injury, a oneto five-year observation period is warranted depending upon severity of cognitive impairment. Careful cognitive evaluation for permanent impairment should then precede medical certification. The presence of blood (hence iron) in the brain parenchyma is thought to play an aetiological role in the development of post-traumatic epilepsy. Simple uncomplicated epidural haematoma without parenchymal blood might allow medical certification following a oneto two-year observation period. Subdural haematoma is often associated with underlying cortical contusion, increasing risk of post-traumatic epilepsy. Significant risk is present in the first two years post injury, though it declines with time. With intraparenchymal haematoma, a two-year period of observation is warranted due to the presence of parenchymal blood. Seizure risk also exists with diffuse axonal injury, and a period of one to two years of observation is appropriate. In such cases, however, an observation period up to five years may be appropriate. Neurological symptoms may include headaches and vomiting related to increased intracranial pressure, seizures, focal neurological deficit related to mass effect or infiltration, cognitive changes, and visual field defects related to pituitary neoplasms. Benign parenchymal growths include ependymoma, choroid plexus papilloma, and colloid cyst (considered a cyst rather than a neoplasm). Though craniopharyngiomas are benign, they may invade adjacent neural tissue and are subject to recurrence. At times there may be residual neoplastic tissue, since complete excision carries the risk of creating a neurological deficit. In such instances, medical certification may be possible, conditional upon satisfactory follow-up with serial imaging studies and current status reports. Posterior fossa neoplasms, which characteristically do not lead to seizures, are an exception. Ordinarily limitations have to be imposed, with certification being conditional on periodic evaluation for tumour recurrence. Eventual recurrence is the rule, though with low grade glial neoplasms this may occur indolently over many years. Seizures are a risk, and subtle neurological impairment depending upon location is an additional concern. These features ordinarily preclude medical certification, though some cases of cure appear in the literature. There may be very rare exceptions following a long recurrence-free and symptom-free interval. Others follow a slowly progressive temporal profile, lending themselves to monitoring measures that can identify the point of compromise to flight safety. Over 90 per cent of affected individuals experience hand tremor, 33 per cent head tremor, 16 per cent voice tremor, and 12 per cent leg tremor. Handwriting, fine movements such as using a screwdriver or threading a needle, and drinking soup from a spoon, may be affected. Treatment with aeromedically acceptable beta-adrenergic blocking medicines is often highly effective. Other agents such as primidone have potential sedating and other central effects, precluding their use in licence holders. Identification of the disorder, exclusion of other potentially serious conditions, and determination of functional impairment may allow immediate medical certification. The disease may progress slowly over many years in some, though disturbingly rapidly in others. Therapeutic agents including carbidopa/levodopa may be acceptable, while the dopamine agonists are unacceptable due to their sedative potential. Levodopa agents may be allowed, but dopamine agonists are prohibited due to their potentially sedating effects. If certification is granted following medical evaluation, it should be conditioned upon periodic re-examination and re-evaluation. If disease progression presents a risk to aviation safety, the Medical Assessment should be revoked. Age of onset is often between age 20 and 40, and there is slight female preponderance. Symptoms are myriad and may include localized sensory disturbances, gait abnormalities, focal motor deficit such as hemiparesis or paraparesis, optic neuritis, speech disturbances, and sphincter disturbances. Symptoms such as vertigo and diplopia would clearly compromise flight safety, while minor paresthesiae in an extremity might be inconsequential. When recovery from an exacerbation has occurred and stability under observation has been documented, medical certification may be appropriate. With minor occurrences, a three-month period of observation may be sufficient, whereas six to twelve months may be more appropriate when more significant disease is present. Single pilot operations, with the prospect of immediate deployment may be disqualifying for certain conditions such as migraine and multiple sclerosis, whereas airline pilot operations may be compatible with certification. Multi-crew operations will often confer an additional measure of risk mitigation, allowing favourable aeromedical dispositions. The same is true for air traffic control duties, where single controller positions can be avoided. Additionally, circumstances may allow assignment to non-safety-sensitive air traffic control duties during a period of observation that might lead to favourable medical disposition. Thus operational considerations may allow some latitude in the medical certification process. Combining these elements with his experience and the evaluation of a neurologist, the medical assessor can arrive at the appropriate aeromedical disposition. The medical examiner should be familiar with the visual requirements for safe flight and other aviation functions such as air traffic control. The ordinary clinical eye examination will be reviewed, and the requirement for special examinations in certain cases will be described. Its main purpose is to serve as a guide in the implementation of the medical provisions of Annex 1. Methods are outlined for the comprehensive evaluation of the visual function of applicants at initial and periodic re-examinations. The aim is to achieve a measure of international uniformity of procedures and results in the assessment of both normal applicants and those in whom there is suspicion or overt manifestation of disturbed visual function or eye disease. To achieve uniformity, therefore, Contracting States shall ensure that equivalence in the methods of evaluation be obtained. An applicant failing to obtain a satisfactory result in such a test shall be assessed as unfit unless able to readily distinguish the colours used in air navigation and correctly identify aviation coloured lights. Applicants who fail to meet these criteria shall be assessed as unfit except for Class 2 assessment with the following restriction: valid daytime only. Both uncorrected and corrected visual acuity are normally measured and recorded at each re-examination. Conditions which indicate a need to obtain an ophthalmic report include: a substantial decrease in the uncorrected visual acuity, any decrease in best corrected visual acuity, and the occurrence of eye disease, eye injury or eye surgery. Single-vision near correction (full lenses of one power only, appropriate for reading) significantly reduces distant visual acuity and is therefore not acceptable. If this requirement is met only by the use of near correction, the applicant may be assessed as fit provided that this near correction is added to the spectacle correction already prescribed in accordance with 6. The Class 3 requirements differ from Class 1 requirement only in Notes 2 and 3 to paragraph 6. When near correction is required, the applicant shall demonstrate that one pair of spectacles is sufficient to meet both distant and near visual requirements. Single-vision near correction (full lenses of one power only, appropriate for reading) may be acceptable for certain air traffic control duties. However, it should be realized that single-vision near correction significantly reduces distant visual acuity. In the flight environment the following factors should be kept in mind because they may reduce visual performance significantly: a) high speed; b) altitude; c) inadequate cockpit illumination; d) glare; e) acceleration; f) vibration; g) poor ergonomics; h) adverse cabin environment.

If extra iron is indicated allergy shots drug names generic 5 mg clarinex with mastercard, a liquid form is protein intake should also be increased and a zinc preferable allergy vaccine cheap clarinex 5mg. It is illogical Opinion is divided as to the merits of daily [31] and probably futile to do the latter without the versus weekly iron administration [32] allergy forecast madison wi buy 5 mg clarinex free shipping. To optimise absorption and occurs in intestinal cells which then cannot absorb minimise nausea allergy forecast topeka ks purchase cheap clarinex, the daily dose should ideally be therapeutic daily doses of iron until they are resplit into two allergy shots yearly order clarinex australia. Some patients find that flavoured newed by cell turnover at roughly 3-day interzinc lozenges allergy forecast portsmouth nh discount 5mg clarinex with mastercard. Constipation can be signiCalcium and vitamin D, osteoporosis ficantly reduced by an increase in fibre intake and and osteopenia appropriate prescription of laxatives and/or stool softeners [22]. This is believed to be 492 Clinical Paediatric Dietetics due to factors such as poor nutrition, delayed recommended if intake of vitamin A from other puberty, reduced levels of mobility and weightsources is significant and provides intakes above bearing exercise, and reduced exposure to sunlight the accepted safe level. It is inappropriate for chilcompromised and/or who rely on nutritional supdren whose skin condition already attracts stares port. If a <2 years who have been receiving a proprietory forlong-term feeding problem seems likely, insertion mula containing it. A liquid evidence of the effects of improved nutrition before formulation of selenium is more practical. Selenium preparations in cause significant periand postoperative oral and combination with vitamin A should not be pharyngeal blistering. In of the patient, the tube used should be as soft and of fact, delaying placement only adds to their stress as narrow a gauge as possible, and it should not be and frustration, engendering increased feelings of re-sited at every feed, but left in situ. Tubes likely to continue with oral nutrition, albeit in small can be secured with a minimally adhesive dresand varying quantities. This is important, not only sing such as Mepiform or tape Mepitac or a nonfor social reasons but also in anticipation of a time, adhesive dressing such as Tubifast, the tube being after the pubertal growth spurt, when they may secured by winding a length of Tubifast around it be able to take sufficient nutrition orally and the where it enters the nostril. Nutrini Multi the ends of the dressing are then tied together Fibre, Nutrini Energy Multi Fibre or Jevity Plus) behind the head. The choice of daytime bolus versus pumped overnight gastrostomy feeds will depend on the individual child and family dynamGastrostomy feeding ics; some prefer a combination. However, difficulties with chewing Painful defaecation with/without (especially meat), compliance with medications constipation and maintenance of a satisfactory fibre intake are issues that are likely to continue. Even a moderately bulky stool can tear nutrition, preferring to rely heavily on gastrostomy the delicate anal skin causing fissuring and extreme feeds. Interthe vicious cycle of pain, conscious ignoring of the estingly, despite negative aspects such as leakage or gastrocolonic reflex and secondary anorexia (Fig. Alternatively, one teaspoon lished and detailed discussions regarding the pros of sugar (anecdotal evidence suggests that brown and cons undertaken before surgery takes place. Lactulose should be prescribed, starting normal, making it more susceptible to acid attack with 2. The removal of badly decayed then progresses onto a diet sufficiently high in teeth from a mouth with limited opening may be fibre to promote comfortable defaecation, the fibre extremely difficult even under general anaesthesia source can be phased out. An increase in especially sucrose, at regular intervals throughout fibre intake is important, however, and a fibre conthe day. The frequency of such foods, especially taining feed (preferably one based on a mixed fibre coupled with the complications noted above, is source) should be introduced, orally or by gastrohighly conducive to the development of dental stomy, but only after the extent of faecal loading has caries. However, comfibre source is extremely successful in normalising promise is possible, and families should be taught stool consistency and frequency of defaecation. It is important to note that, if such restricted to the end of mealtimes and continuous preparations are introduced while the child remains sipping of sugary drinks outside mealtimes disfaecally loaded, problems such as abdominal pain, couraged. Therefore, first, intestas eating and drinking are extremely slow and one inal transit time should be assessed. Then, depending on the degree of faecal loading, this can Oesophageal dilatation and colonic be addressed by giving either a bowel-prep soluinterposition tion such as Klean-Prep as a hospital inpatient, or a strong laxative such as Picolax. However, the pharyngeal and oesophageal Dental aspects mucosae are extremely fragile and may rupture. Dietary Reference Values for Food currently remains a last resort for those whose Energy and Nutrients for the United Kingdom. London: nutritional status cannot be maintained by any the Stationery Office, 1991. References 17 Van den Berghe G Dynamic neuroendocrine responses to critical illness. Berkshire: 9 Ingen-Housz-Oro S, Blanchet-Bardon C, Vrillat M Dystrophic Epidermolysis Bullosa Research Assoet al. Fluoroscopically 28 Seshadri A, Shah A, Bhade S Haematological response guided endoluminal balloon dilatation of esoof anaemic pre-school children to ascorbic acid supphageal stricture due to epidermolysis bulllosa plementation. Clinical, Epi31 Hallberg L Combating iron deficiency: daily admindemiologic and Laboratory Advances and the Findings of istration of iron is far superior to weekly administrathe National Epidermolysis Bullosa Registry. Fatal carHaynes L Nutrition for babies with Epidermolysis Bullosa, diomyopathy in dystrophic epidermolysis bullosa. This includes the chemical composition of tooth enamel in junctional International Network of Dietitians in Epidermolysis epidermolysis bullosa. Approximately 500 children each year Metabolic response to burn injury sustain a major burns injury requiring fluid resuscitation [1,2]. Recent evidence suggests that adults with major burns injuries develop a hypermetabolic state in the first 5 days post-injury. This hypermetabolism Assessment of injury Burns are assessed from an accurate history of the Table 25. This should include the cause of the Type of burn Cause of burn injury, the depth and surface area of the wound and whether there has been any smoke inhalation. The Water Kettle, teapot, cup, mug, bath, saucepan main causes and types of burns injury in children Contact Radiator, iron, oven, hot-water bottle and adolescents are listed in Table 25. ApproximFlame House fire, chip pan, electric/coal fire, ately 70% of thermal injuries sustained by children barbecue under 4 years of age are scalds [3]. Fat Chip pan, oven trays Burn depth is classified as: Chemical Cement, hair dye, cleansing agents, l Partial thickness (superficial, superficial dercytotoxic drugs mal, deep dermal) Electrical Electrical appliances, overhead and l Full thickness underground cables Other Over-exposure to radiotherapy, frostbite, Burns are dynamic injuries that are rarely unianimal manure form in depth and therefore require continual 498 Clinical Paediatric Dietetics is present throughout the acute period and has Table 25. Aims of nutritional support nutritional support to meet these figures, this is the aim of nutritional support is to provide approimpractical. It account of age, weight, total body surface area and is well documented that improved nutritional stapercentage burn surface area, can be calculated at tus in the critically ill patient reduces the likelihood the bedside [15,16]. Any formula is only a guideline and provides a starting point for estimating Factors influencing the nutritional requirements requirements. Frequent reassessment and adjustof a child with a thermal injury are listed in Table ment of requirements are needed for an uneventful 25. Protein requirements Energy requirements Protein requirements for children with burns injuries remain unclear. Losses of lean muscle mass Several researchers have investigated energy and negative nitrogen balance have both been requirements in children with thermal injuries. It has also been suggested that higher protein intakes may have beneficial outcomes in thermally injured Table 25. However, a more recent review by Herndon and Tompkins [6] states that protein Age intakes of 3 g/kg/day may raise urea production Sex without improvement in muscle protein synthesis. Weight Height/length Moderate hypoalbuminaemia is common in chilPre-injury nutritional status dren with thermal injuries and the literature sugCurrent nutritional status gests that this can be well tolerated. Increases in Percentage burn surface area protein provision may be required to correct this. If Thickness of burn the serum albumin level falls too low despite the Grafted area calculated protein requirement being met, then Extent of healing albumin infusions should be considered [22]. Burns 499 Vitamin and mineral requirements sepsis mortality in adult burns patients [28]. Omega-3 fatty acids may improve wound healing this area is still very much under debate as [29]. Glutamine deficiency is known to occur in there are few studies that specifically look at the children with burns injuries, but the significance of requirements for vitamins and minerals in children this is unknown [30]. It can be assumed, however, that have a protective effect on protein synthesis and requirements are increased for certain vitamins tissue repair in adults. Glutamine is also the main and minerals because of their role in the metabolic fuel source for gut enterocytes preserving mucosal pathways of the body. When assessing the requireintegrity and reducing bacterial translocation ments in burns patients, the following should be [31,32]. Arginine is known to have many potential considered: beneficial effects in stressed patients; arginine deficiency has been documented in adults postl Vitamin A may have a role in the prevention of burns injury [33]. Excessive ties in meeting the dietary targets alternative nutrisupplementation may result in a nutritional imbaltional intervention may be necessary. Percentage burn surface area Novel substrates Site of injury Pre-existing clinical conditions these include immune-enhancing nutrients such Previous nutritional status as antioxidants, omega-3 fatty acids, glutamine, Special dietary needs arginine and nucleotides. The limited studies availGastrointestinal function able have focused on their use in adults and recomPain management and sedation mendations have yet to be made regarding their Pyrexia Periods of fasting use in children. Antioxidant therapy (vitamins A, Psychological distress C, E) has been shown to reduce burns and burns 500 Clinical Paediatric Dietetics Major burns (>10%) Table 25. Enteral feeds should then be comYounger children Paediatric enteral feeds; high energy menced as early as possible and balanced against 8 kg up to 30 or 45 kg paediatric enteral feeds; paediatric oral intake. Feeding regimens must imbalances and hyperglycaemia, also require take into account fasting periods related to surgical particularly close monitoring. Further guidance on intervention, dressing changes, physiotherapy and enteral and parenteral nutrition support in children medications. The use of gastrostomy feeding has been reported where Choice of oral and enteral feeds long term enteral nutritional support has been required in burns patients [37]. The choice of feed will vary depending on the Well-recognised complications of enteral feedage of the child, the calculated requirements, ing include increased gastric aspirates and diarany underlying medical condition and the clinical rhoea. Some of the products rate are closely correlated with infection and sepsis available for use in the nutritional management of [38]. Diarrhoea occurs frequently in paediatric paediatric burns patients are outlined in Table 25. However, where possible, minimal has constantly changing nutritional needs related enteral feeds should continue to be infused at a to the healing of their wounds. As the percentage very low rate (as little as 2 mL/hour) to maintain burn surface area changes so the nutritional the brush border integrity of the gastrointestinal requirements should be reassessed. These should be compared with preCalculating requirements admission measurements where available. Achieving requirements l Raised serum levels of C-reactive protein predict sepsis in children with burns injuries [44]. Adjustfore a major burn ments to feeding regimens may be beneficial in l There is no previous medical history of note normalising bowel habit. In these circumstances children exhibit increased body fat stores but no significant increase Method of feeding in lean body mass. This should be monitored closely in children with major burns injuries postAn enteral feeding tube should be passed during discharge. Enteral feeds should commence within 6 hours of admission via this route, until such a time as the child is able to feed orally. Case study Enteral feeds should gradually be replaced by oral intake to meet full nutritional requirements. Good An 18-month-old toddler has sustained a 15% paroral hygiene should be maintained throughout.
Buy genuine clarinex line. HIS NHS Tayside Through the Eyes of Patients - Sensitivity to Operations.