Speman
Kai Spiegelhalder, MD, PhD
- Research Scientist, University of Freiburg Medical
- Centre, Department of Psychiatry and Psychotherapy,
- Freiburg, Germany
If you cannot settle youry disagreeement with the school man health news za exit cheap 60pills speman fast delivery, you may ask for mediattion or forr a due process hearing prostate cancer color purchase generic speman on line. The school must have your written permission before doing any individual evaluation or testing prostate cancer 045 buy generic speman on line. If you disagree with the decision prostrate knotweed wiki discount speman online american express, read Chapter 8 for more information about your procedural safeguards mens health south africa buy discount speman 60 pills. The federal law called the Individuals with Disabilities Education Act says that as the parent of a child with a disability prostate 3 times normal size buy speman master card, you have certain procedural safeguards. Procedural safeguards give parents and schools a set of rules to help them work together. The procedural safeguards also give parents and schools ways to solve problems and settle disagreements. If you have good reason to believe that your child is not receiving a free appropriate public education, you may want to make use of your rights, including your right to mediation, to file a state complaint, and to request a due process hearing. In Florida, this transfer of rights happens when the student turns 18, unless the student has been declared incompetent under state law or has a guardian advocate who has been appointed to make educational decisions. If you do not understand the notice, call the school or appropriate contact right away. If you do not agree with what the notice says, there are steps you can take: First, contact the person named in the notice. The Right to Participate You have the right to help make certain decisions about your child’s education. The school must ask you to participate whenever they hold a meeting related to the identification, evaluation, or placement of your child or to the provision of a free appropriate public education to your child. No matter who asked for the meeting, when you participate, you make it easier for the school to serve your child. When you participate, you will want to: Share information about your child and your child’s needs Listen to and think about what other people are saying Ask questions Keep notes or records about the meeting Share your ideas about what can be done to help your child Make sure you understand what is going to happen next If you need a translator to participate in the meeting, one should be provided for the meeting. Be sure to let the school know before the meeting if you need a translator or an interpreter. Read over your records and the parts of this book that are about the type of meeting you will be attending. Call the school 37 and ask to visit your child’s class and talk to your child’s teachers. Make notes about things you want to say or the questions you want to ask and take them to the meeting. You may also take someone with you to the meeting—such as a friend, relative, or other person who has knowledge of your child and can help you. It is helpful to let the school know when you are bringing someone with you to the meeting. The Right to Give, Not Give, or Withdraw Consent For some actions, the school only has to let you know what they have decided to do or not do (give you notice). You will be asked to sign a form that says you agree to what the school is planning. If the school staff refuses to make the change, they will let you know in writing. The school staff may try to help your child in another way, or they may suggest mediation or ask for a due process hearing. Think carefully about whether to give your consent, because you are making important decisions about your child’s education. Most of the time you and the school staff will be able to work together and agree on what will be done for your child. Remember, for some actions, the school must give you a written notice but does not need your consent. Steps in Solving Problems From time to time, you and the school staff may disagree about what is fair or needed for your child. Some disagreements can be solved easily, while others may take more time and effort. The first step in solving a problem is to make sure that everyone understands the problem. It is often best to ask for a meeting when you don’t understand something or think the school doesn’t understand you. Taking a complaint to someone who cannot make decisions is not a good use of time for you or your child. Dispute Resolution If you and the school district are still not able to agree about what is needed for your child, you may decide to ask for mediation, file a state complaint, or ask for a due process hearing. Mediation, formal complaints, and due process hearings all have the same purpose: to solve problems. They are designed to make sure that children with disabilities receive a free appropriate public education. More information about the dispute resolution methods below and the forms you need to complete if you want to use one of them can be found online at. During a mediation session, a trained and impartial mediator will help you and the school district resolve your disagreement about the identification, evaluation, placement, or free appropriate public education of your child. You may ask for mediation at any time—even at the same time that you file a complaint or ask for a due process hearing. The purpose of mediation is not for one side to win, but for both sides to come to an agreement. The mediation session will give you and the school district a chance to: Talk about the problem Explain your points of view Come to an agreement that is best for your child the mediator will not decide how to solve the problem. The mediator will help you and the school (or district) staff come up with ideas to solve the problem. This can be very important, since your relationship with the school district may last many years. If you and the school district do not reach an agreement through mediation, you may still file a complaint or ask for a due process hearing. Formal State Complaint Parents may also try to solve problems by filing a formal complaint with the Florida Department of Education. If the issue(s) have already been decided through a due process hearing, then the decision cannot be reconsidered through the complaint process. The administrative law judge cannot know the student or be a friend or relative of the family. At the hearing, the administrative law judge will: Listen to you explain what you want and why Look at the school district’s records and your records 41 Listen to people from the school district explain their point of view Listen to the people you chose to help explain your point of view Ask questions After the hearing, the administrative law judge will make decisions based on the laws and rules. The due process hearing is a formal procedure, so, as in court, certain rules apply: You have the right to have a lawyer or other person to help you. It may take up to 45 days (or longer, in some cases) from the time you ask for the hearing to actually have the hearing and get a decision from the administrative law judge. Of course, you and the school district can agree to make a change if you both believe it is a good idea. While you are waiting for the hearing, you will be asked to try to work things out in a meeting called a resolution session. If the school district wants to have a resolution session or wants to go to mediation and you refuse, the hearing will not take place. If the school district is asking for the hearing, they will send you a written notice. In either case, there are many things you need to do to get ready for the hearing. Decide about Getting Help It is important that you know how to present your case at the hearing. Consider having someone, like a lawyer or other advisor, help you get ready and go to the hearing with you. Sometimes a professor in the special education department will be able to help you. Check Time, Place, and Other Details the time and place for the hearing will be set so that you can be there. Collect Evidence At the hearing, you try to prove to the administrative law judge that you are right. Here are some types of evidence you can present: Evaluation reports Letters and emails Samples of your child’s work Tape recordings of any meetings, if applicable Education records Notes Photographs Get Witnesses You may want to have other people help explain your point of view to the administrative law judge. For example, if you use an evaluation report as evidence, the person who wrote the report should be a witness at the hearing. These things will happen in every hearing: You, your lawyer, or your advocate, and the school district staff will be asked to explain the problem and what you want to happen. If you think that something about the hearing is unfair, tell the administrative law judge right away. After the Hearing the administrative law judge will not make the decision during the hearing. The decision should come to you in writing no more than 45 days (or longer, in some cases) after you first asked for the hearing. The administrative law judge’s written report will: List the facts—the things they found to be true Give the reasons for their decisions—the laws or rules that they used State the decisions they have made to solve the problem Both you and the school district get free written copies of this report. You also may ask for a free written or audiotaped, word‐for‐word record of the hearing. You must file a written notice within 90 days of the time the administrative law judge makes a decision. The team will consider the information you have provided, but they may chose not to act on the information for a variety of reasons. If they refuse, they must request a due process hearing to prove that their evaluation is appropriate. The team may use the results to help them make decisions and plans for your child’s education. Discipline of Children with Disabilities Parents and teachers know it is important for schools to be safe and orderly. Since discipline problems make it hard for teachers to teach and for children to learn, all children must obey school rules. Sometimes when a student does not follow school rules, it results in their suspension or expulsion. The following factors determine when a child with a disability may be removed from their current placement for disciplinary reasons and when they must continue to receive services: How long the child is removed from school Whether the child’s misbehavior is a manifestation (result) of the child’s disability 46 Whether the misbehavior involved weapons or illegal substances (such as drugs) or whether there is a good chance of serious bodily injury to the child or others Whether the removal is a change in placement A child with a disability may be removed from their current placement for disciplinary reasons for up to 10 school days in a school year, and for more days for separate acts of misconduct, as long as the removals do not form a pattern. However, if a child with a disability is removed from school for more than 10 days during a school year, the child must continue to receive services that will help them make progress in the general curriculum and toward their annual goals. The chart on the next page describes what the school or district must do when a child with a disability is removed from school for disciplinary reasons. The school must provide services that the student needs to days in a row that would result in a make progress in the general curriculum and toward their annual total of more than 10 cumulative goals. The school must provide services that the student needs to days in a row make progress in the general curriculum and toward their annual goals. If the misbehavior is not due to the student’s disability, the changes of placement. If the misbehavior is due to the student’s disability and a hearing officer determines the student may be dangerous to themselves or others, school personnel will recommend an interim alternative placement to a hearing officer, who makes the placement decision. The Family Educational Rights and Privacy Act and other laws give you many rights related to school records. These rights include: the right to see your child’s records the right to have school records kept confidential the right to ask that school records be changed the right to have a hearing about school records If you believe the school district has violated school records laws, you may file a complaint with the Family Policy Compliance Office of the United States Department of Education at: Family Policy Compliance Office U. You may also have someone else—a friend, relative, or adviser—look at the records if you wish. In any case, the school must show you the records within 30 days of your asking to see them. The school staff will keep a list of the people to whom they have shown or sent your child’s records. This list will include the name of the person, when the person used the records, and why the person needed the records. If someone who is not authorized to see the records wants to see them, the school will ask you to sign a consent form. This form will tell you: Who will get the school records Which school records they will get Why they need the school records Before deciding to sign or not sign the form, you may want to ask: To see the records yourself To talk to the person who wants the records To discuss the records with someone at the school Whether the records will be shown to the person or whether copies will be sent to the person for them to keep the information above is about school records. You can ask to have something: Added to the record Taken out of the record Changed in the record You should ask for any of these actions in writing. The school staff will either do what you have asked or send you a letter telling you they refuse to make that change. The Right to Have a Hearing about School Records You have the right to a hearing if the school refuses to make changes you have asked for in your child’s records. Before asking for this kind of hearing: Be sure that you fully understand what the records say. No matter what is decided at the hearing, you may put a note in your child’s school record to explain your point of view. Note: the school is required to keep a permanent record or specific information about your child for a period of time as defined by the Florida Department of State in General Records Schedule. Once information that is not part of the permanent record is no longer needed to provide educational services to your child, the school district will periodically review it and eliminate information that is no longer useful. It will help you organize information from meetings, notes, and other papers that are part of the process of planning and continuing your child’s education. However, copies of the protocols and testing instruments used to evaluate children are not provided to parents; you will only get copies of the written reports about the results of your child’s evaluations. It will be helpful for you to use an expanding file or three‐ring notebook to hold your child’s records. When you get a new document, you can record the contents on a worksheet in this chapter, if appropriate, and add the document to your file or notebook.
Continuous positive airway pressure as treatment for systemic hypertension in people with obstructive sleep apnoea: randomised controlled trial prostate cancer zytiga purchase speman uk. Effect of continuous positive airway pressure on the incidence of hypertension and cardiovascular events in nonsleepy patients with obstructive sleep apnea: a randomized controlled trial androgen hormone jungle cheap speman 60 pills mastercard. Long-term adherence to continuous positive airway pressure therapy in non-sleepy sleep apnea patients man health customer main customer public discount speman 60 pills. Long-term acceptance of continuous positive airway pressure in obstructive sleep apnea prostate cancer hip pain order speman 60pills online. The impact of a telemedicine monitoring system on positive airway pressure adherence in patients with obstructive sleep apnea: a randomized controlled trial androgenic hormone baldness order speman 60pills free shipping. A Bayesian cost-effectiveness analysis of a telemedicine-based strategy for the management of sleep apnoea: a multicentre randomised controlled trial prostate cancer 8 gleason purchase speman online from canada. A telemedicine intervention to improve adherence to continuous positive airway pressure: a randomised controlled trial. Published by Oxford University Press for the Infectious Diseases Society acute myocarditis, or pericarditis (n = 88) were excluded from of America. Kaplan-Meier survival curves comparing the 30-day readmission (A), cardiovascular mortality (B), and all-cause mortality (C) among people living with human immunodefciency virus admitted with heart failure with reduced ejection fraction who have sleep apnea and an apnea-hypopnea index <24 vs ≥24. Kaplan-Meier survival curves comparing 30-day readmission (A), cardiovascular mortality (B), and all-cause mortality (C) among people living with human immu nodefciency virus admitted with heart failure with reduced ejection fraction who have sleep apnea on continuous positive airway pressure with daily duration of use >4 hours vs ≤4hours. Supplementary Data References Supplementary materials are available at Clinical Infectious Diseases online. Accessed Consisting of data provided by the authors to beneft the reader, the posted 24 September 2017 materials are not copyedited and are the sole responsibility of the authors, 2. Risk of heart failure with human immuno so questions or comments should be addressed to the corresponding deficiency virus in the absence of prior diagnosis of coronary heart disease. Conficts that the editors consider relevant to the con nisms, and clinical cardiovascular consequences. Types and their prevalences, consequences, and presen definitions for cardiovascular endpoint events in clinical trials: a report of the tations. Sleep requiring appropriate cardioverter-defibrillator therapies in patients with conges disordered breathing in patients with symptomatic heart failure: a contemporary tive heart failure. Schulz R, Blau A, Börgel J, et al; Working Group Kreislauf und Schlaf of the J Am Heart Assoc 2013; 2:e000421. Effect of continuous positive airway pressure on the disordered breathing in heart failure with normal left ventricular ejection frac incidence of hypertension and cardiovascular events in nonsleepy patients tion. Effects on sleepiness and quality of life were also demonstrated, provides better evidence for the efficacy of this treatment modality and but improvements in other neurocognitive outcomes were not consistent. Oral Appliances herence is variable with patients reporting using the appliance a median for Snoring and Obstructive Sleep Apnea: A Review. Cartwright has indicated no financial of conflict-of-interest regarding the devices and procedures under conflict of interest. The data for this review were assembled by searching PubMed Address correspondence to: Kathleen A. As for English language peer-reviewed publications containing the sociate Professor of Medicine, Division of Respirology, University of West key words “oral appliance”, “obstructive sleep apnea”, “orth ern Ontario, London Health Sciences Centre, 375 South Street, London, odontic appliances”, and related terms. Articles known to task force members that met the selection ization is a feature of some of these studies, although not always criteria but did not appear in the original search were added to the directed at the outcome of interest. The sures was reported in greater detail than in the earlier literature, elements of this Evidence Table were selected to address the ques probably reflecting an emerging consensus on outcome assess tions in the task force’s charge. These data are contained in an Evi ment and the availability of standardized instruments. What Is the Efficacy of Oral Appliances in the Treatment of Snor their research, but also the types of investigations are much more ing and Obstructive Sleep Apnea in the Short and Long Term? In 80% of the studies, the number Other indicators of improved respiration, such as the minimum of patients who completed the study was between 11 and 50. The oxygen saturation level during sleep showed small increases gen studies differed in the length of time the patient wore the device erally in the range of 1 to 11%. For example, Yoshida47 found a before being re-tested (see Tables 3 and 4) and this may have af significant change in minimum saturation from 72 to 75% and fected follow-up and drop out rates. Reasons for dropping out of Skinner and colleagues46 found an increase from 76 to 82%. Many other studies found an improvement in minimum SaO 4 2 Thus the rates of success may be somewhat inflated in some stud 6,22,28-32,36,37,39,40,43,48,49 or in other measures of oxygenation7,14-16,42 ies as they are reported results based upon those who could toler but these improvements were not always statistically significant. A significant reduction in the number of arousals the number of completed patients, and these success rates might was reported in some studies. Some investi the control of snoring has been less well studied than the con gators approached consecutive patients attending a sleep clinic trol of apnea. Four studies used ob report their findings as the percent of patients reaching 1 or more 6,11,36 jective measurements of sleepiness. Objective measures of daytime sleepiness may provide average rate of success in these studies was 42%. Success rates ranged between 14 and 61% among those sub 56 57 clusal change but not all studies have found this relationship. Several appli the appliance with the greater opening was slightly more effec ances were evaluated in more than 1 study (see Table 3). The effect of the amount of vertical ent inclusion criteria and different treatment protocols may have opening on efficacy and complications is unclear and further in affected the success rates in different studies using the same de vestigations are required. Mehta and coworkers compared of respiratory events between supine and lateral sleep was larger. One long-term per airway size using upright lateral cephalometry with the films study found that weight gain was adversely associated with ef taken during wakefulness. There are also longer-term follow-up studies assessing effective 20,35 Other imaging modalities. A second issue is that the patient characteristics associated Some studies have shown that greater amounts of mandibular with treatment success need to be fully determined. In this study, with an 8-month av for 1 study that employed a compliance monitor (Table 4). All 8 patients were tested with all use on the number of days per week and the number of hours 3 devices. Reasons for non-compliance were severe tongue pain per night the appliance was worn. In 1 study,41 13 of 134 (10%) patients were lost appliance design confound the precise evaluation of side effects to follow up. Two reports used a “2-year follow up” whereas the oth the available research suggests that side effects and complica ers used a mean follow up of 24, 20 and 21. Adherence tions may be grouped as follows: was 100%58,81 in 2 of the studies, while the remaining trials27,82,83 had a median adherence between the first two years of 76% (re 1. These studies also calculated treatment, are minor in severity, tend to resolve in a short adherence based on the reports of patients who completed the period of time or are easily tolerated if they do not resolve study and who were available for follow up. Two of the stud and they do not prevent regular use of the appliance ies58,81 had no dropouts and all patients were available for follow 2. The remaining stage during treatment, are moderate to severe in intensity, studies listed reasons for not completing the study as ineffective tend not to resolve over time and may result in discontinua ness, failed appointments, significant weight loss and appliance tion of appliance use. Loss to follow up was described as due to change in residence, no telephone available and questionnaire not returned. These phenomena were observed in a wide range complete and available for follow up. The reasons for discontinuing appliance use included a range of 0% to 75% of patients. There was no difference Three reports indicated that all compliant patients used the de in the frequency of more severe side effects or complications be vice every night. Two of the studies compared a the patients evaluated for adherence were those who completed non-adjustable, mono-block appliance with an adjustable 2-piece the protocol and were available for follow up. One Two studies evaluated the numbers of hours per night that an other study compared a non-adjustable, mono-block appliance appliance was used by the patient. Many of the minor side effects (discomfort changes were observed after 30 months of treatment with a mean or excessive salivation) improved even with continued appliance 4. However, others are more significant and do not necessarily tion in overbite of a mean 1. Some of the bite changes did not resolve with cessation of relevant, although in some cases they were more pronounced and 85 therapy and more information is needed about the significance therefore of clinical importance. No relationship was found be of these occlusal changes and the risks of long-term appliance tween manifestation of side effects and the degree of protrusion or 57 use. Conceivably, these changes may be due to frank tooth move the initial malocclusion. Additional cephalometric, radiographic and clinical studies vey with 106 agreeing to present for a clinical examination by a 57 are needed to elucidate the importance of these changes. Occlusal changes were assessed using shimstock passed through the occlusion with the patient biting in centric occlusion. Fifteen of the 106 patients (14%) who were clini evaluation in controlled clinical trials. In comparison to the case cally examined after 5 years of treatment had evidence of occlu series reviewed in 1995,3 more recent studies with improved de sal change. In each study, authors found that this approach was effective in many of the the design was a crossover of the 2 treatments with random al cases. Efficacy was compared to baseline at the end dentist is central to the management of this complication and it of treatment periods from 2 weeks to 4 months with 1 to 2 week may be reasonable to continue with treatment in the presence of separation or ‘wash-out’ periods between the treatments. The 2 occlusal change so long as it is not associated with unacceptable most recent studies6,11had substantial numbers of patients, 51 and symptoms, is not overly progressive and that there is adequate 104 respectively. However, failure to respond to conservative well as the consistency of findings, this literature appears valid management, especially if there is loss of posterior support, may and credible. There was little or no effect on change and refuses to abandon the appliance citing that the per other outcomes between the 2 therapies. The occlusion is as and may be single position devices, or partly to fully adjustable. Dental records Some fixed position appliances can be remade with additional are obtained and may include dental radiographs, and a panoramic advancement but this is generally time consuming and needs to survey. Some practitioners obtain a cephalometric radiograph in be done by the dentist or dental laboratory. The rate of modalities including, but not limited to , the polysomnographic advancement and the amount of protrusion is individualized. We did not find studies and the importance of regular, periodic, follow-up examinations. This was first reported in a or others who have undertaken comprehensive training in sleep study that used an appliance that had to be removed from the pa medicine and/or sleep-related breathing disorders with an empha tient’s mouth and adjusted manually. The appliance is advanced either by a hydraulic system92 by individuals who have little or no training and education in this or by remote control. Medical follow-up is also necessary to evaluate treatment response and to assess for recurrence of 3. The appliance may need repairs, adjustments, further ad vancement or even replacement with a different device if side ef 3. No studies have reported on the ideal frequency of the initial cost to the patient includes the cost of the consultation, follow-up visits, but regular assessment in the early weeks and of the dental records needed to manufacture the appliance, and for months of therapy is important to manage side effects, promote the appliance. Cost increases occur when cephalometric radio compliance and reduce the potential for early discontinuation graphs or other dental or airway imaging studies are performed due to any difficulties the patient may have using the appliance. Production costs may vary depending upon plications such as tooth movement, skeletal change or occlusal whether the device is custom-made in a dental laboratory or is an alteration. In this regard, it may be prudent for the dentist to eval off-the-shelf (prefabricated) appliance. Consensus opinion indi uate each patient every 6 months for the first several years and cates that dental laboratory costs for custom-made devices may annually thereafter to ensure the integrity of the oral structures. Service fees can vary greatly depending Tooth movement and malocclusion are noted in some patients on the clinical protocol, actual time spent caring for the patient, especially after 1 or more years of treatment but the occlusal and geographical economic factors. The dentists were found to adjust the appliances Published literature now provides evidence for the efficacy of overall an average of 2. The newer titratable appliances may improve outcomes but fully as many studies reported results based primarily upon those optimal treatment protocols need to be defined. In particular, the subjects who could adapt to the appliance and who returned for role of home monitoring in the optimization of the amount of clinical follow-up. Treatment adherence is variable with a Practice parameters for the treatment of snoring and obstructive median appliance use of 77% of nights at 1 year (by self-report). Am J Respir Crit Care Med 166, 743 pliance or uvulopalatopharyngoplasty in patients with obstructive 748. Sleep able oral appliance for the treatment of mild to moderate obstructive Medicine 1, 299-305. Am J Respir Crit Care Med 166, (1994) Efficacy of a Herbst mandibular advancement device in ob 855-859. Chin J Dent Res 2, tients with obstructive sleep apnoea: a randomized cross-over trial. Sleep 23, S172-178 uvulopalatopharyngoplasty in the treatment of obstructive sleep ap 34. Acta Otolaryngol 119, 503-509 the effect of a mandibular advancement device on apneas and sleep 17. Swed Dent J 23, 117-126 structive sleep apnea : long-term effects on apnea and sleep. A prospective randomized 1-year follow-up Role in the treatment of obstructive sleep apnea. Chest 113, 992-996 effects of an oral device to treat snoring and obstructive sleep apnea.
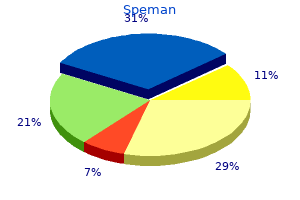
The figure shows three cur rently available screening options with important characteristics such as sensitivity prostate revive buy generic speman 60 pills on line, screening interval prostate jewelry cheap speman uk, and requirement for triage tests [25] ritagoreti26@gmail mens health 4 day workout 60pills speman sale. However man health urban athlon cheap speman 60pills mastercard, the extent to which triage tests are needed differs among the algorithms prostate 9 complex reviews buy cheap speman 60pills. Several other biomarkers prostate wikipedia order speman 60 pills without a prescription, such as p16/Ki-67 cytology or host and viral methylation testing, are currently being evaluated and could become integral parts of screening and management algorithms in the future [20, 21]. The evaluation of any new triage tests would follow the same guiding principle of similar manage ment for similar risk described above for primary screening. A triage test is evalu ated based on its ability to stratify a population into higher and lower-risk groups. The former requires further intervention/follow-up; the latter requires none or a lesser degree of intervention/follow-up (Fig. With so many options available for cervical cancer screening and management, choosing the optimal strategy can be a challenge. Decisions about cervical cancer screening must balance the benefit of preventing cervical cancer with the potential harms and cost of screening. Consideration must be given to the number of women screened to detect one with cancer, the number of screening tests over each wom an’s lifetime, the requirement for triage tests for an abnormal screen, unnecessary colposcopy referral, and the potential for overtreatment. The availability of many tested and proven choices for cervical cancer screening allows for designing new screening programs that adapt to specific needs in different healthcare systems, rather than just incrementally updating successful, but not necessarily efficient, pro grams. On the other hand, the number and complexity of options may be confusing to providers and could increase the risk that women may be lost to follow-up [22 ]. In a particular practice or geographic setting risk assessment, in conjunction with risk modeling and comparative effectiveness, research plays a central role in deter mining the optimal strategies for cervical cancer screening and management. With different preventive options available, many countries are considering a variety of combinations, and no single “winning strategy” has yet emerged. Current risk-based benchmarks used in cervical cancer screening and management are largely based on established practice from cytology based screening programs. It is conceivable that other risk thresholds will be explored in the future, weighing benefits and harms differently to address specific individual and public health needs. In cervical cancer screening, risk thresholds determine whether referral to colposcopy or treatment is needed and what time intervals should be chosen for different screening and management options. It can serve as a reference that allows making test-independent screening and management recommendations. A systematic assessment of benefits and risks to guide breast cancer screening decisions. From differences in means between cases and controls to risk stratification: a business plan for biomarker development. Comparison of three management strategies for patients with atypical squamous cells of undetermined significance: baseline results from a randomized trial. Results of a randomized trial on the management of cytology interpreta tions of atypical squamous cells of undetermined significance. A randomized trial on the management of low-grade squamous intraepithelial lesion cytology interpretations. American Cancer Society guideline for the early detection of cervical neopla sia and cancer. Reassurance against future risk of precancer and cancer conferred by a negative human papillomavirus test. Human papillomavirus and cervical cancer: bio markers for improved prevention efforts. Focused rescreening prior to report issuance, an enhanced quality control measure. The Tahoe study: bias in the interpretation of Papanicolaou test results when human papillomavirus status is known. Barton Grossman Department of Clinical Biochemistry, Royal Infrmary of Department of Urology, the University of Texas M. Fritsche Central Hospital, Finland Department of Laboratory Medicine, the University of Texas M. These To prepare these guidelines, the literature relevant to the use guidelines are intended to encourage more appropriate use of tumor markers was reviewed. An explanation of the methods causes of false-positive tumor marker results that must also be used when developing these guidelines has previously been taken into account (eg, heterophilic antibody interference, high published (2) and has been included as an Appendix to this dose hooking) have previously been published (3). Some patients initially present with upper probably refects the increasing number of cases of hepatitis C abdominal pain, weight loss, early satiety, or a palpable mass in infection (8,9) and liver cirrhosis (10), both strong predisposing the upper abdomen (31). Risks of biopsy combined with ribavirin or other drugs such as lamivudine) are include tumor spread along the needle track (1%-2. There is ongoing debate about the relevance of tifcation of tumors when they are still potentially curable. The much greater disease heterogeneity seen in ally, randomized, controlled trials should be carried out to more advanced disease complicates the selection of optimal demonstrate the effcacy of screening in terms of decreased treatment, which in turn is refected in the considerable varia disease-related mortality and improved survival and cost effec tion in survival rates reported in randomized, controlled trials tiveness (28). Below, we present a more detailed rable objective responses, fewer sessions needed (52) and better discussion of some of the markers listed in Tables 1 and 2. Palliative treatments in advanced disease include arterial chemoembolization, with survival advantages in well-selected candidates (47). Ideally, reference values should be established for each assay, because there is some between-method variation in results. In 117 patients with initially elevated serum prognosis, even after attempted curative resection (70). Incomplete resection yields sured every 3 months for 2 years, and then every 6 months (135). After liver transplantation, follow-up necessarily indicate complete clearance of the disease. These data were later microarray analysis of surgical liver samples from patients confrmed immunohistochemically (196,197). The diagnosis is usually established who have metastatic disease require systemic chemotherapy by cystoscopic evaluation, prompted by hematuria or urinary with multiple anticancer agents (229). In some cases, urine cytology is ing of cancer progression pathways facilitates development of positive for tumor cells. Bladder cancer is staged according to drug therapies against specifc tumor targets (225). Car the majority of bladder cancer patients are diagnosed cinoma in situ (stage Tis) and stages Ta and T1 are grouped as with nonmuscle invasive tumors. Even though these tumors nonmuscle invasive bladder cancers because they are restricted can be completely resected, there is a high risk of recurrence; to the inner epithelial lining of the bladder and do not involve 50%-70% of these patients will develop tumor recurrence the muscle wall. However, because of their high false-positive rate, confdence in the estimate of effect and is likely to change the these tests are not suffciently accurate to be used for screening estimate; D = very low (any estimate of effect is very uncer or early detection of bladder tumors. Several studies have shown that the diagnosis of patients at risk of or with symptoms of bladder UroVysion may also be useful for monitoring patients after cancer (255). In selected patients and when lack of consensus about what constitutes a positive result (228). According to one recent report, the test has a sensitivity of 81% and specifcity of 75% in detecting bladder cancer (258). However, Tumor Markers in Bladder Cancer 21 the performance of this marker in early stage bladder cancer urinary tract (283). With each cell cycle, the ends of the telomeres shorten, until a critical length is reached after the protein survivin is an inhibitor of apoptosis that is associ which cell division leads to breakdown of the telomere. Telomerase is inactivated in nor tissues but high in cancer tissues and transformed cell lines mal human epithelial tissue, but is reactivated in neoplasia (291). More recently, Sha authors reported 62% sensitivity and 96% specifcity for telom riat et al reported sensitivity and specifcity and positive and erase activity in exfoliated urothelial cells (280). The most common genetic change seen tumor tissue, have been proposed to be associated with a favor in bladder cancer is loss of heterozygosity in chromosome 9. All of these reports suggest that microsatellite analysis of Other Proposed Markers exfoliated cells is potentially useful to detect bladder cancer. Detection of hypermethylation of promoter regions lite polymorphisms for bladder cancer detection, demonstrated of tumor suppressor genes and apoptosis genes also appears to sensitivity of 58% and specifcity of 73% for detection of recur have potential diagnostic value for bladder cancer (324-326). The work-up of patients with hematuria is 100% and a specifcity of 89% for detection of these high-grade costly and may require cytology, cystoscopy, intravenous urog bladder tumors in 139 patients (308). In this study, 267 unnecessary cystoscopies be analyzed in urine cells by noninvasive methods (347,348). The high false-positive rate is the major Role of Urine Markers for Patient criticism of the urine-based tests when they are used to assess Surveillance patients who present with hematuria or are used in patient sur veillance. The urine markers used in patient surveillance have on occa sion been criticized for their low sensitivity in detecting disease Role of Tissue Markers for Prognosis (351,352), but in most studies they have signifcantly improved Considerable research continues to be directed toward the the detection of bladder cancer when used in conjunction with identifcation of markers that predict the aggressive potential cytology and cystoscopy. It appears that urine sive treatment of those patients with tumors most likely to markers can assist in the early detection of recurrence in patients progress to invasive or metastatic disease (336). The objective of such Although many studies have demonstrated that the preva panel testing should be to improve both the sensitivity and the lence of p53 alterations in bladder cancer increases with stage specifcity for bladder cancer detection. Cervical cancer progresses testing can improve the effcacy of cervical cancer screening. In developing countries, screening cer precursor lesions and cervical cancer, primary prevention facilities are not readily available and most women present with of (pre)malignant cervical disease is feasible. Large tumors may present with data of the bivalent and quadrivalent vaccines demonstrate vaginal discharge. Screening effcacy against cervical cancer will require long-term follow techniques include conventional Papanicolau smears or liquid up in clinical trials (372,373). However, with radical surgery, 25 26 Use of Tumor Markers in Liver, Bladder, Cervical, and Gastric Cancers ovarian function can be preserved and vaginal stenosis sec with recurrent disease and poor survival (358,374,382-384). Therefore, most patients with early cal cancer declines dramatically from approximately 80%-95% stage cancer will be treated by radical hysterectomy and pelvic in patients without lymph node metastases to approximately lymphadenectomy. In these cases, it has been reported gested that tumor markers may be helpful in the management that concomitant chemoradiation with platinum-based chemo of patients with cervical cancer(eg, in predicting prognosis, in therapy signifcantly improved disease-free survival and sur selecting high-risk patients who need adjuvant treatment, and in vival compared with radiotherapy alone (375,376). The role of chemotherapy in patients with recurrent or cervical adenocarcinoma (414-419). There is no cutoff point that is specifc for Sensitivities for lymph node metastases of 58%, 45%, and 23% cervical malignancy. How diation were better than pretreatment serum concentrations in ever, in contrast with other reported investigations, lymph node predicting clinical outcome (413). Incidence is highest in those both 5-fuorouracil and radiation therapy compared with a group patients older than 60 years, and marked geographical varia of patients given 5-fuorouracil alone (457), several other stud tions have been observed. Risk factors include Helicobacter ies have shown that concurrent chemo and radiotherapy are pylori infection, atrophic gastritis, male sex, cigarette smok superior to chemotherapy alone, although combination therapy ing, high salt intake, and some of the genetic factors associated has shown more morbidity (458,459). Surgery is the only potentially curative that postoperative adjuvant chemotherapy and chemoradio treatment, but even when surgical resection is possible, long therapy gave improved disease-free survival and survival rates term survival occurs only in a minority of patients, with overall (464). If a D2 resection is not performed there is a signifcant about 300,000 individuals, sensitivity of this test for gastric risk of understaging (448,453,480). In multivariate are at considerable risk of gastric cancer and indicated a need analysis, however, their impact is not always independent of for consensus as to best practice (475). Additional markers that have been stud of the American College of Gastroenterology (476). Conventional cytologi measured by conventional imaging techniques (507,508) and cal examination of intraoperative peritoneal lavage fuid is use may be useful in the detection of recurrence. Although the number of investigations is limited, confrmation within appropriately designed clinical trials. Risk factors for hepatocellular carcinoma 1990, pp 168 among patients with chronic liver disease. Niederau C, Fischer R, Sonnenberg A, Stremmel W, Trampisch for the use of tumor markers. Fattovich G, Giustina G, Degos F, Tremolada F, Diodati G, agement, and treatment of hepatitis C: An update. Guidelines for the diagnosis and treatment of hepato Gastroenterology 1997;112:463-472. Diagnostic evaluation of hepatocellular carcinoma in groups and preventive strategies. Gastroenterology screening for detection of small hepatocellular carcinoma in 1986;90:263-267. Colombo M, de Franchis R, Del Ninno E, Sangiovanni A, De hepatic arteriovenous shunting due to hepatocellular carcinoma Fazio C, Tommasini M, et al. Hepatocellular carcinoma in Ital and cirrhosis, and its change by transcatheter arterial emboliza ian patients with cirrhosis. Hepatoma with severe non-islet cell tumor hypoglyce cases of hepatocellular carcinoma at a Western center. Cancer 1986;58:2485 of randomized trials for hepatocellular carcinoma treated with 2488. Tumor markers in primary malignanciesof the ous biopsy before surgical resection of hepatocellular carcinoma. The evolution of pathologic features of hepa preanalytical, analytical and biological sources of variation and tocellular carcinoma. Intention-to-treat analysis of asparagine-linked sugar chains of alpha-fetoprotein purifed surgical treatment for early hepatocellular carcinoma: resection from human ascites fuid. Saitoh S, Ikeda K, Koida I, Suzuki Y, Kobayashi M, Tsubota macol Ther 2006;23:1535-1547. The usefulness of simultaneous determinations of glucosami Semin Liver Dis 1999;19:323-328. Glycan composition of serum alpha-fetoprotein in patients Food and Drug Administration approval of oncology drugs.
These antibiotics provide unique solutions for your research needs androgen hormone treatment speman 60pills on-line, such as dual selection and rapid mens health 4 day workout generic 60pills speman, stable cell line establishment prostate cancer drugs buy genuine speman on-line. Geneticin Selection Antibiotic Geneticin reagent prostate cancer youtube quality speman 60pills, also known as G418 sulfate prostate 30 grams discount 60pills speman visa, is commonly used for the selection of mammalian prostate cancer 60 buy speman now, plant, or yeast cells. The higher purity of Geneticin reagent means that 15–30% lower concentrations are required compared to other G418 products; therefore, surviving clonal colonies may arise faster, and cells appear healthier. Zeocin Selection Antibiotic Zeocin reagent is effective in mammalian cell lines, yeast, insect cells, and bacteria. The concentration required for selection ranges from 50 to 2,000 μg/mL (typically 300 μg/mL), depending on the cell type. Hygromycin B Selection Antibiotic Hygromycin B is an aminoglycosidic antibiotic that inhibits protein synthesis by disrupting translocation and promoting mistranslation of the 80S ribosome. Because its mode of action is different from Geneticin or Zeocin reagents, hygromycin B can be used in dual‑ selection experiments. The concentration for selection ranges from 100 to 1,000 μg/ mL (typically 200 μg/mL), and should be optimized for each cell line. Puromycin Dihydrochloride Selection Antibiotic Puromycin, a translation inhibitor in both prokaryotic and eukaryotic cells, is an aminonucleoside antibiotic from Streptomyces alboniger. Resistance is conferred by the puromycin N‑acetyltransferase gene (pac) from Streptomyces. Puromycin has a fast mode of action, causing rapid cell death even at low antibiotic concentrations, allowing the generation of puromycin‑resistant stable cell lines in less than one week. Adherent mammalian cells are sensitive to concentrations of 2–5 μg/mL, while cells in suspension are sensitive to concentrations as low as 0. Cell death occurs rapidly in cells sensitive to blasticidin, and blasticidin‑ resistant, stable mammalian cell lines can be generated in less than one week at low antibiotic concentrations. Reporter Gene Assays Reporter genes are genes whose products can be readily assayed subsequent to transfection, and can be used as markers for screening successfully transfected cells, for studying regulation of gene expression, or serve as controls for standardizing transfection efficiencies. The ideal reporter gene should be absent from the cells used in the study or easily distinguishable from the native form of the gene, assayed conveniently, and have a broad linear detection range. It is also important that the presence of the reporter gene does not affect the normal physiology and general health of the transfected cells. Generally, reporter gene assays are performed 1–3 days after transfection; however, the optimal time for the assay should be determined empirically. Transfection assays In contrast to selectable markers, which protect an organism from a selective agent that would normally kill it or prevent its growth, reporter genes used for screening transfectants make the cells containing the reporter gene visually identifiable. Reporter genes used in this way are normally expressed under their own promoter independent from that of the introduced gene of interest, allowing the screening of successfully transfected cells even when the gene of interest is only expressed under certain specific conditions or in tissues that are difficult to access. For example, transfection efficiencies between different experiments can be normalized by comparing the expression levels of a reporter gene used in all of the experiments. Gene regulation assays Reporter gene assays are invaluable for studying regulation of gene expression, both by cis‑acting factors (gene regulatory elements) and trans‑acting factors (transcription factors or exogenous regulators). Furthermore, reporter gene systems enable the use of pathway‑ specific, tissue‑specific, or developmentally regulated gene promoters as biomarkers for specific events or processes. In these assays, the detectable reporter gene acts as a surrogate for the coding region of the gene under study. Upon introduction of the reporter construct into cells, expression levels of the reporter gene are monitored through a direct assay of the reporter protein’s enzymatic activity. Common reporter genes Commonly used reporter genes that induce visually identifiable characteristics usually involve fluorescent and luminescent proteins. Yellow and red versions are also available, allowing the investigation of multiple genes at once. The luciferase enzyme catalyzes a reaction with its substrate (usually luciferin) to produce yellow‑green or blue light, depending on the luciferase gene. Since light excitation is not needed for luciferase bioluminescence, there is minimal autofluorescence and thus virtually background‑free fluorescence. It has become a prominent tool for protein knockdown studies, phenotype analysis, function recovery, pathway analysis, in vivo knockdown, and drug target discovery. Next, this cleaved message is targeted for degradation, which ultimately results in the loss of protein expression. Likewise, both are important targets for therapeutic use because of the roles they play in the controlling gene expression. Occurrence Whether or not they occur naturally in mammals is an unsettled question. Note that while the basics of transfection experiments share certain similarities, conditions vary widely depending upon the cell type used for transfection. Therefore, we recommend that you familiarize yourself with the cell line of interest and the appropriate transfection method, and closely follow the instructions provided with each product you are using in your experiments. Factors Influencing Transfection Efficiency Successful transfection is influenced by many factors—the choice of the transfection method, health and viability of the cell line, number of passages, degree of confluency, quality and quantity of the nucleic acid used, and the presence or absence of serum in the medium can all play a part in the outcome of your transfection experiment. While it is possible to optimize specific transfection conditions to achieve high transfection efficiencies, it is important to note that some cell death is inevitable regardless of the transfection method used. Cell type the choice of which cell type to use for a transfection experiment may seem obvious, but it is a critical factor that is often overlooked. Since each cell type is likely to respond differently to a given transfection reagent or method, choosing the appropriate cell type and proper experimental design are necessary to maximize results. While established continuous cell lines are easier to work with in the laboratory, they may not be the best choice for modeling in vivo processes because of the multiple genetic changes that they have undergone. However, if the purpose of the transfection experiment is high-level production of recombinant proteins, it is not important that the cell line represents the in vivo situation as long as the cell line can express sufficient quantities of recombinant proteins with proper folding and posttranslational modifications. For example, transient transfection of suspension-adapted Expi293F cells grown in Expi293 Expression Medium enables researchers to produce, starting from the vector of interest, greater than 1 g/L of correctly folded and glycosylated recombinant proteins. Primary cultures, on the other hand, are often used because they more closely mimic natural tissues. However, they typically have a limited growth potential and life span, and are more difficult to maintain in culture. When using primary cultures, it is important to maintain a largely homogeneous population of cells (for example, neuronal cultures should be enriched for neurons and suppressed with regard to glial cells) and use the cells as soon as practical. In addition, biological properties of the cell type must be taken into consideration when designing transfection experiments. For example, some promoters function differently in different cell types and some cell types are not well suited to particular transfection technologies. Transfection efficiency in cancer cell line panel 100 Lipofectamine 3000 80 Lipofectamine 2000 60 40 20 0 Cell line Figure 6. Each condition was tested in triplicate, and the data points show the mean transfection efficiency plus standard deviation. Cell health and viability the viability and general health of cells prior to transfection is known to be an important source of variability from one transfection to another. In general, cells should be at least 90% viable prior to transfection and have had sufficient time to recover from passaging. We strongly recommend subculturing cells at least 24 hours before transfection to ensure that they recover from the subculture procedure and are in optimum physiological condition for transfection. Cell cultures with immortalized cell lines evolve over months and years in the laboratory, resulting in changes in cell behavior with regard to transfection. Excessive passaging is likely to detrimentally affect transfection efficiency as well as total transgene expression level from the cell population as a whole. In general, we recommend using cells that have undergone less than 30 passages after thawing of a stock culture. Thawing a fresh vial of frozen cells and establishing low-passage cultures for transfection experiments allow the recovery of transfection activity. For optimal reproducibility, aliquots of cells of a low passage number can be stored frozen and thawed as needed. Since contamination can drastically alter transfection results, cell cultures and media should be routinely tested for biological contamination (see Biological Contamination, page 14), and contaminated cultures and media should never be used for transfection. If cells have been contaminated or their health is compromised in any way, they should be discarded and the culture reseeded from uncontaminated frozen stocks. Confluency For optimal transfection results, follow a routine subculturing procedure and passage cultures once or twice a week at a dilution that allows them to become nearly confluent before the next passage. The optimal cell density for transfection varies for different cell types, applications, and transfection technologies, and should be determined for every new cell line to be transfected. Maintaining a standard seeding protocol from experiment to experiment ensures that optimal confluency at the time of transfection is reliably achieved. With cationic lipid–mediated transfection, generally 70–90% confluency for adherent cells or 5 × 105 to 2 × 106 cells/mL for suspension cells at the time of transfection provides good results. Make sure that the cells are not confluent or in stationary phase at the time of transfection, because actively dividing cells take up foreign nucleic acid better than quiescent cells. Too high of a cell density can cause contact inhibition, resulting in poor uptake of nucleic acids and/or decreased expression of the transfected gene. However, too few cells in culture may result in poor growth without cell-to-cell contact. In such cases, increasing the number of cells in culture improves the transfection efficiency. Similarly, actively dividing cell lines are more efficiently transduced with viral vectors. Media Different cells or cell types have very specific medium, serum, and supplement requirements, and choosing the most suitable medium for the cell type and transfection method plays a very important role in transfection experiments. Information for selecting the appropriate medium for a given cell type and transfection method is usually available in published literature, and may also be obtained from the source of the cells or cell banks. If there is no information available on the appropriate medium for your cell type, you must determine it empirically. It is important to use fresh medium, especially if any of the components are unstable, because medium that is missing key components and necessary supplements may harm cell growth. For cell culture media information, see Media recommendations for common cell lines, page 28, or refer to our website (thermofisher. The quality of serum can significantly affect cell growth and the transfection result. Therefore, it is important to control for variability among different brands or even different lots of serum to obtain best results. After testing the serum on your cells, keep using the same serum to avoid variation in your result. Our products, including sera, are tested for contamination and guaranteed for their quality, safety, consistency, and regulatory compliance. Antibiotics In general, antibiotics can be present in the medium for transient transfection. However, because cationic lipid reagents increase cell permeability, they may also increase the amount of antibiotics delivered into the cells, resulting in cytotoxicity and lower transfection efficiency. Avoiding antibiotics when plating cells for transfection also reduces the need for rinsing the cells before transfection. For stable transfections, penicillin and streptomycin should not be used in selective medium, because these antibiotics are competitive inhibitors of the Geneticin selective antibiotic. When creating stable cell lines, allow 48–72 hours after the transfection procedure for cells to express the resistance gene before adding the selective antibiotic. If using serum-free medium, use lower amounts of antibiotics than you would in serum containing medium to maintain the health of the cells. Transfection method There are a number of strategies for introducing nucleic acids into cells that use various biological, chemical, and physical methods. However, not all of these methods can be applied to all types of cells and experimental applications, and there is a wide variation with respect to transfection efficiency, cell toxicity, effects on normal physiology, level of gene expression, etc. The ideal approach should be selected depending your cell type and experimental needs, and should have high transfection efficiency, low cell toxicity, minimal effects on normal physiology, and be easy to use and reproducible. For an overview and comparison of various transfection methods, see Gene Delivery Technologies, page 46. Use the tables below to choose between the various cationic-lipid transfection reagents and the Neon Transfection System available from Thermo Fisher Scientific. For more information on each transfection method, as well as optimized protocols for the transfection of wide range of cell lines, go to thermofisher. However, because these cells have undergone genetic transformation to become immortalized, their behavior in culture may not necessarily reflect the in vivo situation. Primary cells and finite cultures Primary cells are isolated directly from the tissue and proliferated under appropriate conditions. As such, they are morphologically and physiologically more similar to an in vivo state. However, they are usually more difficult to culture and transfect than continuous cell lines. Therefore, their phenotype is intermediate between primary cells and continuous cultures. The use of such cells is sometimes easier than the use of primary cells, especially for the generation of stably transfected clones. Expression in mammalian cells Invitrogen™ ViraPower™ Expression Systems use replication-incompetent viral particles to ensure safe and highly efficient delivery of expression constructs for high-level constitutive or inducible expression in any mammalian cell type. The kits have two versions: kits for high-accuracy titer, allowing for precise control of copy number per cell, or kits for fast titering, which are ideal for high-throughput screening studies. This system is ideal for expressing toxic proteins, because the inducible promoter allows the control of the timing of gene expression. The ViraPower™ Adenoviral System uses Gateway Technology for fast, easy, and accurate cloning of the gene of interest. For more information on ViraPower expression systems as well as on other expression systems not discussed here, go to thermofisher.
Cheap speman generic. 2 Upper Back Exercises For Strengthening With Resistance Bands.
