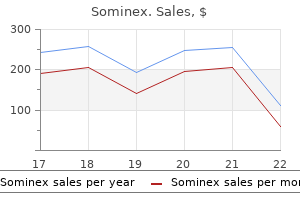
Sominex
Caleb P. Bupp, M.D.
- Department of Medical Genetics
- Spectrum Health System
- Grand Rapids, Michigan
When possible sleep aid vital nutrients buy generic sominex 25mg online, If the mother has untreated early syphilis at delivery sleep aid 3 ingredients cheap generic sominex canada, 10 a full 10-day course of penicillin is preferred sleep aid vape order generic sominex line, even if ampicil days of parenteral therapy can be considered sleep aid 99 cent only 25 mg sominex fast delivery. The use of agents Scenario 3 other than penicillin requires close serologic follow-up to assess adequacy of therapy sleep aid non addictive purchase generic sominex pills. In all other situations insomnia you are not my friend cheap sominex online amex, the maternal history Infants who have a normal physical examination and a of infection with T. Passively transferred maternal Older infants and children aged 1 month who are identi treponemal antibodies can be present in an infant until age fed as having reactive serologic tests for syphilis should have 15 months; therefore, a reactive treponemal test after age 18 maternal serology and records reviewed to assess whether months is diagnostic of congenital syphilis. If the nontrepone they have congenital or acquired syphilis (see Primary and mal test is nonreactive at this time, no further evaluation or Secondary Syphilis and Latent Syphilis, Sexual Assault or Abuse treatment is necessary. This treatment also would Penicillin Shortage be adequate for children who might have other treponemal infections. During periods when the availability of penicillin is com promised, the following is recommended (see. For infants with clinical evidence of congenital syphilis seroreactive at delivery) should receive careful follow-up (Scenario 1), check local sources for aqueous crystalline examinations and serologic testing. Ceftriaxone must response after therapy might be slower for infants treated after be used with caution in infants with jaundice. Terefore, ceftriaxone should be used in consultation who have had a severe reaction to penicillin stop expressing pen with a specialist in the treatment of infants with congenital icillin-specifc IgE (238,239). Penicillin skin testing with the major and at age 6 months if the initial examination was abnormal. For infants without any clinical evidence of infection at high risk for penicillin reactions (238,239). Although these (Scenario 2 and Scenario 3), use reagents are easily generated and have been available for more a. For premature infants who have no other clinical evidence accompanying minor determinant mixture. One approach suggests that persons Management of Persons Who with a history of allergy who have negative test results should be regarded as possibly allergic and desensitized. Another Have a History of Penicillin Allergy approach in those with negative skin-test results involves test No proven alternatives to penicillin are available for treating dosing gradually with oral penicillin in a monitored setting in neurosyphilis, congenital syphilis, or syphilis in pregnant women. Readministration of penicillin to these patients outpatient-monitored test doses can be considered. Because anaphylactic reactions to penicillin can be fatal, every efort should be made Penicillin Allergy Skin Testing to avoid administering penicillin to penicillin-allergic patients, unless they undergo acute desensitization to eliminate anaphy Patients at high risk for anaphylaxis, including those who lactic sensitivity. Skin-test reagents for identifying persons at risk for adverse reactions to penicillin* skin-test reagents before being tested with full-strength reagents. Beall and test is positive if the average wheal diameter after 15 minutes Annals of Internal Medicine. Intradermal Test Diseases Characterized by If epicutaneous tests are negative, duplicate 0. The margins of the Urethritis, as characterized by urethral infammation, can wheals induced by the injections should be marked with a ball result from infectious and noninfectious conditions. An intradermal test is positive if the average wheal if present, include discharge of mucopurulent or purulent diameter 15 minutes after injection is >2 mm larger than the material, dysuria, or urethral pruritis. Asymptomatic infections initial wheal size and also is >2 mm larger than the negative are common. Although the two approaches have not been compared, with drug regimens efective against both gonorrhea and oral desensitization is regarded as safer and easier to perform. Further testing to determine the specifc etiology Patients should be desensitized in a hospital setting because seri is recommended because both chlamydia and gonorrhea are ous IgE-mediated allergic reactions can occur. Oral desensitization protocol for patients with a positive skin test* trachomatis (197). Documentation of chlamydial infection Note: Observation period was 30 minutes before parenteral administration is essential because of the need for partner referral for evalua of penicillin. Enteric bacteria have been identifed as an uncom and sex partners referred for evaluation and treatment. Such patients should be treated with drug regimens efective against Clinicians should attempt to obtain objective evidence of gonorrhea and chlamydia. However, if clinic-based diagnostic cally should be evaluated and treated, if indicated. The Gram stain is the preferred chlamydia is strongly recommended because of the increased rapid diagnostic test for evaluating urethritis and is highly utility and availability of highly sensitive and specifc testing sensitive and specifc for documenting both urethritis methods. However, because men Treatment should be initiated as soon as possible after diag with documented chlamydial or gonococcal infections have nosis. Azithromycin and doxycycline are highly efective for a high rate of reinfection within 6 months after treatment chlamydial urethritis; however, infections with M. Expedited partner treatment and patient Erythromycin ethylsuccinate 800 mg orally four times a day for 7 days referral are alternative approaches to treating partners (71). Persons who have persistent or be instructed to abstain from sexual intercourse for 7 days after recurrent urethritis can be retreated with the initial regimen single-dose therapy or until completion of a 7-day regimen, if they did not comply with the treatment regimen or if they provided their symptoms have resolved. Persistent urethritis for reinfection, men should be instructed to abstain from sexual after doxycycline treatment might be caused by doxycycline intercourse until all of their sex partners are treated. If compliant with the initial regimen and re-exposure can be excluded, the fol Follow-Up lowing regimen is recommended while awaiting the results of Patients should be instructed to return for evaluation if symp the diagnostic tests. Symptoms Recommended Regimens alone, without documentation of signs or laboratory evidence of urethral infammation, are not a sufcient basis for retreatment. A four-glass Meares-Stamey lower-urinary diagnosis of gonococcal cervical infection, it is not a sensitive tract localization procedure (or four-glass test) might be helpful indicator, because it is observed in only 50% of women with in localizing pathogens to the prostate (255). Estimates vary When an etiologic organism is isolated in the presence considerably depending on the source and sensitivity of the of cervicitis, it is typically C. Limited data indicate that infection If men require treatment with a new antibiotic regimen with M. For reasons that are unclear, cervicitis the suspected cause, all partners in the past 60 days before the can persist despite repeated courses of antimicrobial therapy. Because the sensitivity of microscopy (commonly referred to as mucopurulent cervicitis or cervicitis) to detect T. Several factors should affect the decision to provide presumptive therapy for cervicitis or to await the results of Management of Sex Partners diagnostic tests. Expedited partner treatment and patient referral (see For women in whom any component of (or all) presumptive Partner Management) are alternative approaches to treating therapy is deferred, the results of sensitive tests for C. Women who receive such therapy should return infectious disease in the United States, and prevalence is high after treatment so that a determination can be made regard est in persons aged 25 years (93). To detect chlamydial infections, health-care provid Follow-up should be conducted as recommended for the ers frequently rely on screening tests. If symptoms persist, sexually active women aged 25 years is recommended, as is women should be instructed to return for re-evaluation because screening of older women with risk factors. Recent evidence to recommend annual chlamydia screening of sexually active suggests that the liquid-based cytology specimens collected for women aged 25 years. Among Treating infected patients prevents sexual transmission of women, the primary focus of chlamydia screening eforts the disease, and treating all sex partners of those testing positive should be to detect chlamydia and prevent complications, for chlamydia can prevent reinfection of the index patient and whereas targeted chlamydia screening in men should only be infection of other partners. Treating pregnant women usually considered when resources permit and do not hinder chlamydia prevents transmission of C. An appropriate sexual Chlamydia treatment should be provided promptly for all per risk assessment should be conducted for all persons and might sons testing positive for infection; delays in receiving chlamydia indicate more frequent screening for some women or certain treatment have been associated with complications. The following recommended treat urethral infection in men can be made by testing a urethral ment regimens and alternative regimens cure infection and swab or urine specimen. Unlike the test-of-cure, which is not recommended, to treat patients for whom compliance with multiday dosing repeat C. The clinical signifcance and transmissibility of men should be a priority for providers. Erythromycin might be less efcacious than either azithromycin or doxycycline, mainly Patients should be instructed to refer their sex partners for because of the frequent occurrence of gastrointestinal side evaluation, testing, and treatment if they had sexual contact efects that can lead to noncompliance. To minimize Among heterosexual patients, if concerns exist that sex disease transmission to sex partners, persons treated for chla partners who are referred to evaluation and treatment will mydia should be instructed to abstain from sexual intercourse not seek these services (or if other management strategies are for 7 days after single-dose therapy or until completion of a impractical or unsuccessful), patient delivery of antibiotic 7-day regimen. To minimize the risk for reinfection, patients therapy to their partners can be considered (see Partner also should be instructed to abstain from sexual intercourse Management). Compared with standard partner referral, until all of their sex partners are treated. Abstinence should be continued until 7 days after successfully could yield false-positive results because of the a single-dose regimen or after completion of a multiple-dose continued presence of nonviable organisms (197). Pregnant Doxycycline, ofoxacin, and levofoxacin are contrain women aged <25 years are at high risk for infection. The results of one study involving a limited number of patients suggest that a short Recommended Regimen course of azithromycin, 20 mg/kg/day orally, 1 dose daily for 3 days, might be efective (292). Erythromycin base or ethylsuccinate 50 mg/kg/day orally divided into 4 doses daily for 14 days Topical antibiotic therapy alone is inadequate for treatment of chlamydial infection and is unnecessary when systemic Follow-Up treatment is administered. Follow-up of infants is recom approximately 80%, a second course of therapy might be mended to determine whether the pneumonia has resolved, required. Terefore, follow-up of infants is recommended although some infants with chlamydial pneumonia continue to to determine whether initial treatment was efective. Mothers of infants who have chlamydia pneumonia and Management of Mothers and Their Sex Partners the sex partners of these women should be evaluated and The mothers of infants who have chlamydial infection and treated according to the recommended treatment of adults for the sex partners of these women should be evaluated and treated chlamydial infections (see Chlamydial Infection in Adolescents (see Chlamydial Infection in Adolescents and Adults). In addition, peripheral eosinophilia (400 cells/ treatment is not indicated, and the efcacy of such treatment is mm3) occurs frequently. Sexual abuse must be considered a cause of chlamydial Diagnostic Considerations infection in preadolescent children, although perinatally trans Specimens for chlamydial testing should be collected from mitted C. Tissue culture is the defnitive standard for tract, and rectum might persist for >1 year (see Sexual Assault chlamydial pneumonia. However, because of lower sensitivity, a negative Gram stain should not be considered sufcient for ruling out infection in asymptom other Management Considerations atic men. In addition, Gram stain of endocervical specimens, See Sexual Assault or Abuse of Children. The majority specimen types including endocervical swabs, vaginal swabs, of urethral infections caused by N. Although widespread screening is not recommended compromised by cross-reaction with nongonococcal Neisseria because gonococcal infections among women are frequently species. For Because nonculture tests cannot provide antimicrobial sexually active women, including those who are pregnant, susceptibility results, in cases of suspected or documented Please note: An erratum has been published for this issue. Health departments should prioritize partner notifcation cline and azithromycin, routine cotreatment might also hinder and contact tracing of patients with N. Extensive clini have decreased susceptibility to ceftriaxone, and 48 isolates cal experience indicates that ceftriaxone is safe and efective had decreased susceptibility to cefxime. In 2008, no isolates for the treatment of uncomplicated gonorrhea at all anatomic demonstrated decreased susceptibility to ceftriaxone; cefxime sites, curing 99. To ensure appropriate antibiotic therapy, clinicians utility of having a simple and consistent recommendation for should ask patients testing positive for gonorrhea about recent treatment regardless of the anatomic site involved. In published clinical trials, the axetil 1 g orally in treating pharyngeal infection is poor (56. However, it has been efective oral cephalosporins) for treating gonococcal infections of the in published clinical trials, curing 98. Providers should inquire about oral sexual exposure urogenital and anorectal gonococcal infections. Spectinomycin and if reported, treat these patients with ceftriaxone because has poor efcacy against pharyngeal infection (51. Azithromycin 2 g orally is efective against uncomplicated Single-dose injectible cephalosporin regimens (other than gonococcal infection (99. None of the recommended because several studies have documented treat injectible cephalosporins ofer any advantage over ceftriaxone ment failures, and concerns about possible rapid emergence of for urogenital infection, and efcacy for pharyngeal infection antimicrobial resistance with the 1-g dose of azithromycin are is less certain (306,307).
Diseases
- Teebi Shaltout syndrome
- Onychonychia hypoplastic distal phalanges
- Developmental dysphasia familial
- Chromosome 3, trisomy 3p
- Ainhum
- Chondrosarcoma (malignant)
After edema has been present for some time sleep aid 2 cheap generic sominex canada, areas of brown pigmen Etiology tation (hemosiderin and melanin) may appear sleep aid non prescription order sominex without a prescription. X6 Legs Chronic sleep aid trazodone discount sominex 25mg otc, but dependent on stage of insufficience and reaction on causal therapy sleep aid 25mg doxylamine succinate uk discount sominex 25mg. Pain Quality: the intermittent pain is cramping and severe and arises insomnia nutrition buy sominex amex, usually insomnia 2012 discount generic sominex canada, after fixed Page 135 and consistent amounts of exercise. Laboratory Finding Arteriography demonstrates the level of arterial obstruc Code tion or obstructions. Recurrent or chronic limb pain due to inappropriate use of muscle groups whether or not for References psychological reasons may be quite common. In chronic cases bad body mechanics, lordosis or scoliosis, trauma, and arthritis are the most common Code causes. Xla Post-traumatic gia are similar in all regions and are normally unilateral and limited to one or two dermatomal segments. Definition Paroxysmal pain in the distribution of an intercostal Site nerve commonly associated with cutaneous tenderness Pain classically is in the precordium, although radiation in the affected dermatome. Post-traumatic Associated Symptoms intercostal neuralgia often has continuous pain with ex As noted, pain is aggravated by stress and relieved acerbation. Frequently patients also experience breathlessness, sweating, nausea, and Etiology belching. Usually it is very Usual Course severe and lasts several hours or until relieved by mor Anginal pain typically is brief and intermittent, brought phine. Complications Signs and Laboratory Findings Arrhythmia and myocardial infarction may occur. Physical examination may be normal but may show hy pertension, S3 or S4 gallop rhythm, and papillary muscle Social and Physical Disability dysfunction with a mitral regurgitant murmur, as well as If angina is brought on by little extra stress, there is seri signs of forward or backward cardiac failure. Recovery frequently takes several months, and physical and psychological complications may prolong Code recovery and affect not only the patient but family mem 324. If dissection occurs, sudden and on chest X-ray if there is an effusion, as well as changes severe pain occurs, maximal at onset. Page 140 Signs and Laboratory Findings Site A discrepancy may develop between pulses or blood Diaphragmatic pain is deep and difficult to localize. A new aortic regurgitant Noxious stimulation may affect phrenic nerve sensory murmur may develop. Acute Main Features complications include acute aortic valvular incompe the pain is deep, dull, poorly localized, and non-specific tence, occlusion of major vessels, hypotension, and if it involves only the central chest and upper abdomen death. Social and Physical Disability the main problems with aortic aneurysms are life and Associated Symptoms death considerations. Arteriosclerosis are, the most classic would be elevation of a hemidia is a major cause. Usual Course Differential Diagnosis There is usually a specific therapy once the etiology is Angina, pulmonary diseases, and thoracic disk disease. These relate partly to the underlying disease process and partly to the vagueness of understanding of the cause of pain. Social and Physical Disability If the tumor is inoperable and the patient cannot eat, a Differential Diagnosis plastic tube can be passed through the tumor or a feeding Involves a wide range of cardiac, pulmonary, muscu jejunostomy performed. X2 Infection: gastrointestinal source Summary of Essential Features and Diagnostic 453. Definition Chronic pain at the costal margin which may mimic vis Main Features ceral pain. The condition may be bilat usually dysphagia without pain, which usually occurs eral. Rising from a sitting position in an armchair is show a dilated esophagus; barium swallow, a narrowing often a particularly painful stimulus. Site Relief Anterior thorax, axilla, medial upper arm; usually one Restriction of movement may give relief. Pain Quality: often burning, intensified by touch Physical activities are often restricted by pain or fear of or clothing. Reduction in apprecia teria tion of pinprick, cold, and touch related to the incision A fairly common condition which should be considered and upper arm. X6 Summary of Essential Findings and Diagnostic Cri teria References Pain commencing postoperatively, usually immediately, Copeland, G. Differential Diagnosis Postmastectomy Pain Syndrome: Herpes zoster, local infection, radiation necrosis in ribs, recurrent neoplasm. Differential Diagnosis Site Herpes zoster; pleurisy related to infection; and second Spine, thorax at site of cancer, arms. There may also be a is more protracted, with onset more than five years after pleuritic component to the pain. Complications Associated Symptoms Patients with skeletal, visceral, and brachial plexus dam If the thoracotomy was done for tumor resection and age have a short survival of less than one year. Page 144 Usual Course most frequently associated with sharp, spontaneous If the pain is due to traumatic neuromata, it usually de pains radiating to the chest, axilla, or neck. If the pain is due to tumor recurrence, some relief may be ob Associated Symptoms tained by an intercostal nerve block or radiation therapy. The patients usually do not tolerate contact with clothing or the water of the shower. There may be tenderness to Main Features percussion or to palpation of the upper abdomen. A barium swallow teria may show disordered esophageal contractions with or Epigastric discomfort and esophageal reflux are key without `spasmor esophageal dilatation. X6 Abdominal pain cial pressure devices in the esophagus for 24 to 48 hours may pick up very high pressure contractions, which may be related to the pain. Most pa Attacks of severe pain, usually retrosternal and midline, tients with motility disorders run a benign course with due to a diffuse disorder of the esophageal musculature occasional attacks of pain. Pain is usually well localized to the midline behind the sternum, between the epigastrium and the suprasternal Complications notch. Age of Onset: occurs in young adults Severe pain may restrict normal activities and be so and middle aged. This is mainly a physiologic rather than a pathologic the bouts are usually infrequent. There is a sensation of the food retrosternal pain which may be relieved by nitrites, with sticking in the lower part of the esophagus. The diagnosis is made with a of gravity, the weight of the food causes the sphincter to combination of barium swallow appearances and disor open when the patient rises from the chair, and the stick Page 148 dered esophageal motility and normal mucosal appear Code ances on esophagoscopy. Main Features Prevalence: common in young adults and middle age Main Features group, starting in third decade. Sex Ratio: more common Prevalence: common, especially in middle aged and in females, especially in the obese or during pregnancy. Pain Qual Time Pattern: bouts of pain occur often after postural ity: burning retrosternal pain, especially at night if lying changes such as bending over or lying down. There may be iron-deficiency Aggravating Factors anemia and positive occult blood tests. Esophageal motility stud Social and Physical Disability ies may show a decrease in cardiac sphincter pressure, a Unable to tolerate certain foods, unable to sleep flat in pH probe may detect acid reflux, and the pain may be bed. Pathology Changes in the lower esophageal mucosa may vary from Summary of Essential Features and Diagnostic the mildest changes with blunting of the rete papillae to Criteria severe hemorrhage inflammation with ulceration and Burning retrosternal pain from esophageal inflammation. Page 149 Complications Gastric Ulcer with Chest Pain Patients with ulceration may develop a stricture in the region of the ulcer which can cause dysphagia. Site Laboratory Findings Unilateral in the abdomen, usually confined to a single None diagnostic but a chest X-ray, intravenous urogram, dermatome. Main Features Initially there is abdominal wall pain, which is sharp and Complications burning but intermittent. With nerve entrapment in the rectus sheath the pain oc Pathology curs, or is made worse, when the abdominal wall is No histological abnormality identified in ribs. It is as tensed, for example if the patient is asked to raise the sumed that the cause is irritation of an intercostal nerve head and neck off the examining couch. Treatment Reassure the patient of the benign nature of the condi Differential Diagnosis tion. The pain of appendicitis is present even when Renal or ureteric pathology, spinal problems, pulmonary the abdomen is relaxed and usually is associated with pathology. Bowel ischemia may Right upper quadrant, but also epigastrium and other also be a factor. Main Features System Dull aching pain in association with a tender enlarged Gastrointestinal; gallbladder and bile duct. Sex Ratio: much more common in Physical findings of congestive heart failure may include women. Definition System Right upper quadrant pain in patients following chole Gastrointestinal system. Main Features Site Sex Ratio: males and females are about equally affected, Right upper quadrant. At first may be periodic Prevalence: this pain is a common occurrence soon after and infrequent, every two to three months lasting for a the gallbladder has been removed, often with a short few days. Pain commonly responds to regular antacid and Complications anticholinergic therapy and particularly to H2 receptor Risk of analgesic addiction or further unnecessary sur antagonists, but there is a high incidence of relapse. Social and Physical Disability Recurrent or chronic pain will restrict normal activities Code and reduce productivity at work. Social and Physical Disability Summary of Essential Features and Diagnostic Cri Restriction of normal activities and reduction of produc teria tivity at work. Occurs at any age but commonly in young and middle aged adults and is still more common in men. Periodic Main Features pain, which commonly lasts from a few days to two or Uncommon, occurring predominantly in middle-aged three weeks, with pain-free periods lasting for months. Dyspepsia and often nausea occur, but vomiting which is not relieved by antacids, to a constant dull pain. The diagnosis is made on endoscopy or intestinal bleeding, hematemesis and/or melena, or signs barium meal (upper gastrointestinal series). Pain commonly responds to appro Physical findings include those of obvious weight loss of priate doses of antacids and healing is promoted by H2 cachexia, a palpable mass in the epigastrium, and an receptor antagonists. Laboratory findings are mainly of ane relapse, which can be considerably prevented by main mia, which may be microcytic due to chronic blood loss, tenance doses. Pain can vary from a dull discomfort to , in the Occult blood is commonly present in the stool. Generalized symptoms of fatigue, anorexia, weight loss, fever, and depression occur early in the course of the Usual Course disease. The patient may present with a sudden onset of If the patient presents early in the course of the disease diabetes mellitus late in life, without a family history, or the tumor may be resectable, although the chance of with recurrent venous thromboses. Complications There may be obstruction at the cardia or pylorus, or Signs and Laboratory Findings metastases in the liver or in more distant organs such as Evidence of recent weight loss and eventually cachexia the lungs or bone, resulting in bone pain. Jaundice and a central or lower epigastric hard mass are late findings, and a palpable spleen tip is Social and Physical Disability uncommon. Usual Course Only a minority of patients, from 20 to 40%, are oper Summary of Essential Features and Diagnostic Cri able at the time of diagnosis. The overall prognosis even Central or paraumbilical or upper abdominal over the with modern imaging techniques is poor. Definition Main Features Pain due to chronic granulomatous disease of the gastro Progressively severe abdominal pain precipitated by intestinal tract. Associated Symptoms There may be symptoms suggestive of gastric or duode System nal ulceration or intermittent incomplete small bowel Gastrointestinal system, sometimes including liver. Signs and Laboratory Findings There may be evidence of generalized atherosclerosis as Main Features shown by absent femoral popliteal or pedal pulses, or the Becoming increasingly common in young adults but can presence of an epigastric bruit. Arteriographic evaluation colicky central abdominal pain in bouts; or localized indicates severe stenosis or occlusion of all three mesen inflammation (abscess formation) may cause a constant teric vessels, including the inferior mesenteric artery, the severe pain. Intestinal obstruction associated with distention, nausea and vomiting, alteration in bowel habit, constipation or Usual Course diarrhea or both, aggravated by eating, relieved by Progressive weight loss and abdominal pain if untreated. Summary of Essential Features and Diagnostic System Criteria Gastrointestinal system. Abdominal pain, usually dull, sometimes exacerbated by eating due to chronic constipation, which is largely a Main Features disorder of Western civilization and increases with age. The pain is located over the cutaneous markings of the colon, most Differential Diagnosis commonly in the left lower quadrant and upper abdomen Diverticular disease, carcinoma of the colon. The pain may vary from being constant and dull to sharp or very severe, but it never Code prevents sleep. Diverticular Disease of the Colon More common in females, with ratio varying from 2:1 to 5:1. Males and fe tal examination and on sigmoidoscopy at rectosigmoid males are equally affected. Barium enema shows colonic ated with acute inflammation (acute diverticulosis), and spasm; a small percentage are lactose intolerant. Palpable descending the pain can be incapacitating and result in deterioration and sigmoid colons with or without tenderness. Page 158 Summary of Essential Features and Diagnostic Cri Social and Physical Disability teria Surgical treatment may involve a permanent colostomy. A common chronic condition of the elderly resulting in constipation, colonic distension, and sometimes abdomi Pathology nal pain. The diagnosis is made by identification of di the pathology is that of adenocarcinoma, beginning in verticuli on barium enema. Most commonly lower abdominal or perineal pain from a lesion of the rectosigmoid area.
Purchase sominex 25 mg with mastercard. Sleep: A bedtime story.
He found that the healing rate was six times greater comparing movement and exercise with immobility in patients with articular cartilage defects sleep aid homeopathic order sominex uk. Articular cartilage defects in rabbits that were immobilized caused 50% of them to develop arthritis at one year insomnia yahoo answers trusted 25 mg sominex. Prolotherapy stimulates the and statistically significant protective natural healing mechanisms of the body via effect on prevention of progressive inflammation sleep aid vape sominex 25mg discount. Salter showed by x-ray and clinical findings that the animals that received exercise did much better than the ones who were immobilized sleep aid using pumpkin seeds cheap sominex 25 mg. One of the great things about Prolotherapy is that movement is encouraged during the treatment course insomnia 46 order sominex pills in toronto. Those who are sedentary use this as an opportunity to change their lifestyles in order to maximize healing sleep aid with no side effects best purchase for sominex. Joint injuries requiring the patients to limit weight-bearing, require adaptation of the rehabilitation programs, but not complete rest by any means. We utilize a number of exercises that are non-weight-bearing, but get the patients moving and even increase their heart rates so that fitness can be maintained, or achieved if the patients were previously sedentary (often due to the injury. Because we are athletes ourselves, we know the importance of daily physical activity for overall health and well being. We provide individualized physical activity and rehabilitation programs for all of our Prolotherapy patients at Caring Medical and work closely with them to achieve their goals, adapting the workouts as needed. Continuous passive motion exercise was also shown to heal or clear a hemarthrosis (blood in the joint) twice as fast as immobilized limbs. The notion that the area must be iced and compressed to decrease swelling is outdated. Bleakley reported that ice seemed to be more effective at limiting swelling and decreasing pain in the short-term, immediately after injury; however the long-term effects on tissue repair seemed to indicate that evidence is limited and outcome has not been shown to improve with use of ice post injury. This involves exercise and proteolytic enzymes, which help clean out the damaged tissue. Exercise or passive motion by a physical therapist or on your own at home is tremendously effective at helping resolve the bleeding and edema but will also aid the healing process. Animals continue their activities after an injury, therefore they heal well after an injury. They go through the inflammatory cascade, just as if the body received Prolotherapy! Because the body has its own type of Prolotherapy which is the inflammation that occurs after an injury. When cells burst open from the trauma, D-glucose and cytokines are released from inside the cell, platelets change their shape to stop the bleeding and release growth factors such as platelet-derived growth factor and fibroblastic growth factor and the arachidonic acid from the lipid layer of the cells eventually is turned into various prostaglandins. This inflammatory reaction sends a signal to the brain that a four-alarm injury is occurring in this location and we need resources! Remember, pain is a blessing because it tells the body there is a problem that needs to be fixed. The Science Behind Prolotherapy Normal muscle tissue (prior to Muscle tissue 96 hours after an Muscle tissue 96 hours after an Prolotherapy). This is the Prolotherapy was presented at the annual Prolotherapy solution known Clinical Symposium of the Prolotherapy Association, June 16, 1968, Bellevue Hotel, as P2G. The various solutions, when injected into the injured area, induce the normal inflammatory cascade to help heal such tissues as ligaments, tendons, discs, and cartilage. Rheumatoid arthritis is a systemic inflammatory condition and treatment involves use of medications that inhibit tumor-necrosis factor such as Enbrel and Humira (or generics etanercept and adalimumab) which have been shown to enhance quality of life and slow the arthritic process. Consider the fact that in rheumatoid arthritis you went from giving patients high dose steroids and methotrexate (chemotherapy drug) to these tumor-necrosis factor inhibitors. Rheumatoid arthritis is a systemic disease affecting the whole the Many Benefts of Joint Swelling body. In rheumatoid arthritis, which involves joint swelling, an increase in cytokines, such as tumor-necrosis factor and interleukin-1, occurs in the joint fluid. Therefore, modern medicine uses drugs to block these substances thinking that the joint swelling will be reduced and hopefully the amount of articular cartilage breakdown will also be reduced. In rheumatoid arthritis this has been successful, except the articular cartilage still breaks down. You see, the advent of these medications, though more sophisticated, is still producing the same old story: modern therapeutics believing the savior for joint pain is going to be a drug, when clearly the cause of the disease and the propagation of the joint swelling is joint instability! Treatment should be geared at repairing the cause of the joint swelling, not the chemistry of the joint swelling! Use of more sophisticated drugs such as interleukin-1 blockers or corticosteroid injections (or for that matter, interleukin injection blockers) just limit joint swelling for a longer period of time, but you leave the joint vulnerable to further injury and degeneration. Swelling helps to disperse the forces on the joint in an attempt to protect the joint structures, including the medial cartilage. Taking anti-inflammatories while maintaining athletics and activities can become a devastating combination. Without the joint swelling, stretching the ligaments, which then activates nerve endings within the ligament, the body has no idea that the joint is breaking down. So as your joint is breaking down, you feel no pain because you have taken these medications. Many of our patients do deep water running, which is one of the best ways to get motion without stress. We tell our patients to feel the injured joint before and after exercise and compare it to the uninjured side. When the joint swells from inflammation, it will feel warm compared to the uninjured side; thus joint swelling is a great indication to guide not only exercise and activity, but also therapies. Injection solutions can be modified to stimulate healing, but not promote more pain and swelling. As for more severe injuries, Prolotherapy can speed up healing many-fold, and our athletes typically do not want to be out of competitions for months, so they come in for Prolotherapy treatments right away. Swelling in the joint is also a guide as to how much exercise to do and how to proceed. We ask our athletes to check the temperature of the injured joint before, during, and immediately after exercise. It is definitely possible for an athlete to experience setbacks just because of pushing the exercise too much after an injury. After an injury or after Prolotherapy do not push exercise to the point where the joint feels hot. New heat sensations in the joint means the joint is swelling because the activity or exercise put the joint in a compromised, unstable position which will inhibit, not help healing! So you can see, receiving treatments that stop joint swelling could have major devastating effects on joints that would clearly promote osteoarthritis, not slow its progression! The injured person has two choices: change the chemistry that is causing the joint swelling or treat the cause of the chemical changes which cause the joint instability. Without treating the joint instability, even if modern medicine comes up with a medication concoction that blocks 80 of the 100 substances that cause joint swelling, there will still be 20 left because the cause of the joint swelling will remain. The best way to approach life is to always solve the underlying cause of the problem vs a band-aid approach. These band-aids, even if seemingly successful at slowing the degenerative cascade, (though this is not true in most cases), allow the underlying disease process to continue. Once the joint swelling is eliminated, the patient can exercise without hesitancy for the rest of his life. As we have been reiterating in this chapter, the body heals by the process of inflammation. Taking medications that stop inflammation will subsequently stop the body from healing. Interestingly enough, the reason arthritis forms in the first place is because an injured area did not heal. The pain of the initial injury may have been relieved by taking a medication that blunted the symptoms, but the injured tissue remained injured, as manifested by decreased strength. In a study where dogs were exercised for one year carrying jackets weighing 130% of their body weight, all knee joints were inspected for evidence of joint injury and degeneration at the completion of the study. Articular cartilage surfaces from the medial tibial plateau were examined by light microscopy, the cartilage thickness was measured, and intrinsic material properties were determined by mechanical testing. Furthermore, the tibial articular cartilage thickness and mechanical properties did not differ between the exercised group and non-exercised group. These results show that a lifetime of regular weight-bearing exercise in dogs with normal joints did not cause alterations in the structure and 18 mechanical properties of articular cartilage that might lead to joint degeneration. The worst things for healing an injury are to take anti-inflammatories and receive cortisone injections. There are numerous studies showing the deleterious effects of anti-inflammatories, such as ibuprofen, on healing. Ibuprofen, the prototype anti-inflammatory medication, has been shown to have an inhibitory effect on bone healing, remodeling, resorption, and metabolism. The proteoglycan concentration of the cartilage matrix was also 26,29 suppressed significantly. Radiographic analysis was done yearly with an average length of follow up being three years. By the third year of the study, the results were so dramatic demonstrating the acceleration of the degeneration of the articular cartilage in the osteoarthritic knee patients that this part of the study had to be stopped. There were more than twice as many patients showing deterioration in the indomethacin group as the placebo. Interactions occur between prostaglandin metabolism, inflammatory proteins, and bone metabolism. Systemic as well as local source of inflammation appear to be actively involved in both bone formation and resorption. This study showed that early administration of ibuprofen in the postoperative period was detrimental to tendon healing. Thus this shows that ibuprofen should also not be used when treating acute 37 tendon injuries. Use of this product poses a significant risk in accelerating osteoarthritis joint breakdown. Instead of recommending Prolotherapy for continued complaints of pain, the usual course of treatment is perhaps the most potent of all anti-healing therapies: the cortisone shot. Receiving a cortisone shot is one of the quickest ways to lose strength at the ligament-bone junction (fibro-osseous junction or enthesis). Cortisone and other 40 steroid shots have the same detrimental effects on articular cartilage healing. Corticosteroids inactivate vitamin D, limiting calcium absorption by the gastrointestinal tract and increasing the urinary excretion of calcium. Bone also shows a decrease in calcium uptake, ultimately leading to weakness at the fibro-osseous junction (enthesis). Corticosteroids also inhibit the release of Growth Hormone, which further decreases soft tissue and bone repair. Although anti-inflammatory Figure 2-13: Known effects of intraarticular corticosteroids on articular cartilage. The steroid shots induced a tremendous amount of damage including chondrocyte necrosis (cartilage cell damage), hypocellularity (decreased number of cells) in the joint, decreased proteoglycan content and synthesis, and decreased collagen synthesis in the joint. Even after one steroid injection, cartilage remained biochemically and metabolically impaired. Other studies have confirmed similar harmful effects of steroids on joint and cartilage tissue. Figure 2-15 explains the monumental difference between cortisone and Prolotherapy injections. Corticosteroids are often used to treat tendon injuries but may also be associated with tendon ruptures and impaired healing. Article title: Effects of intraarticularly administered corticosteroids and salicylates on the pool and leading to surface structure of articular cartilage. The problem with cortisone is that immediate pain relief is possible, but in reality it may be permanently reducing the ability to remain active. They then go onto the playing field with severe injuries that required cortisone shots to relieve the pain. The injury Cortisone Versus Prolotherapy will, unfortunately, never heal because of the tremendous anti Cortisone Prolotherapy healing properties of cortisone.
Weed (Marijuana). Sominex.
- Stimulating appetite in people with AIDS.
- Are there any interactions with medications?
- Treating multiple sclerosis (MS).
- How does Marijuana work?
- Dandruff, hemorrhoids, obesity, asthma, urinary infections, leprosy, preventing rejection after kidney transplants, and other conditions.
- Are there safety concerns?
- Treating increased pressure in the eyes (glaucoma).
- What is Marijuana?
- Dosing considerations for Marijuana.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96910