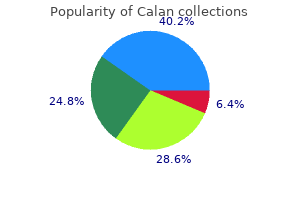
Calan
Jean Heather Hoffman-Censits, M.D.
- Co-leader, Women�s Bladder Cancer Program, Greenberg Bladder Cancer Institute
- Assistant Professor of Oncology

https://www.hopkinsmedicine.org/profiles/results/directory/profile/10004183/jean-hoffmancensits
Second arteria japan discount 80mg calan with amex, the items tended to focus on minor details rather than on more relevant scien tifc concepts heart attack normal blood pressure buy calan from india. For each numbered statement blood pressure 5040 buy calan australia, choose A if increase in the first is accompanied by increase in the second or if decrease in the first is accompanied by decrease in the second B if increase in the first is accompanied by decrease in the second or if decrease in the first is accompanied by increase in the second C if changes in the first are not necessarily accompanied by changes in the second 1 arteria lumbalis buy calan with visa. Because the items could include only absolutely true or false facts arrhythmia khan academy purchase calan canada, K-type items could not be used to assess clinical judgment except in comparisons arteria epigastrica superior effective calan 80mg. Tus, they could appear too complicated and require the test-taker to constantly keep the answer code in mind. In addition, the possible response combinations introduced a cueing efect that decreased item discrimination. Sample K-type item Directions Summarized A 1, 2, 3 only 1, 3 only 2, 4 only 4 only All are correct A child experiencing an acute exacerbation of rheumatic fever usually has: 1. Foundational science items should not be answerable based simply on clinical knowledge alone or on pattern recognition (for example, providing a list of symptoms and asking what drug to prescribe). Tese items should require clinical knowledge and also knowledge of one or more foundational science principles that would have likely been learned in pre-clinical education and hopefully reinforced during clinical rotations. Patient Care: Diagnosis Causes and Mechanisms Identifes the cause/causal agent or predisposing factor(s) or, given an efect, determines the cause. Identifes the underlying processes/pathways that account for, or contribute to , the expression or resolution of a given condition. Recognizes the mechanisms of action of various drugs; selects from an option set list of drugs based on mechanism of action. Patient Care: Diagnosis Obtaining and Predicting History and Physical Examination Knows signs/symptoms of selected disorders. Given current symptoms in presented history, identifes pertinent factor in the history. Given a specifc problem, knows what to ask to obtain pertinent additional history. The response options should not be referenced in the vignette and should not include details that would be obtained during initial history-taking. If asking about information that was already obtained and is mentioned in the vignette, use the following lead-in. Patient Care: Diagnosis Selecting and Interpreting Laboratory and Diagnostic Studies Selects most appropriate laboratory or diagnostic study, including neuropsychiatric testing, or study most likely to es tablish/confrm the diagnosis. Selects most appropriate laboratory or diagnostic study afer change in patient status. Patient Care: Diagnosis Determining Prognosis/Outcome Recognizes factors in the history, or physical or laboratory study fndings that afect patient prognosis or outcome, or that determine therapy. Interprets laboratory or other diagnostic study results and identifes current/future status of patient. Recognizes associated conditions of a disease, including complications, or indicators of potential complications. Recognizes characteristics of disease relating to natural history or course of disease, including progression, severity, duration, and transmission of disease for a specifc patient. Knows pertinent incidence statistics and identifes patient groups at risk; knows incidence of symptomless/dangerous disorders among various groups. Knows common screening tests for conditions amenable to prevention or detection in an asymptomatic patient or population. Knows appropriate counseling (and reassuring, comforting) of patient or family regarding current and future prob lems, including risk factors related to present encounter. The response options focus on features and course of disease as they relate to a specifc patient. Patient Care: Management Selecting and Monitoring Pharmacotherapy Selects most appropriate pharmacotherapy. Assesses patient adherence to treatment regimen, recognizes techniques to increase compliance with or understand ing of the disease state, and knows how adherence may be afected by providing instructions with therapy. Response options are factors about the patient that afect the choice of a drug regimen. Knows adverse efects of various drugs or recognizes signs and symptoms of drug (and drug-drug) interactions re sulting from polypharmacy in the therapeutic regimen, and knows steps to prevent polypharmacy including labora tory studies to monitor drug therapy. Knows modifcations of a therapeutic regimen within the context of continuing care. Knows appropriate monitoring to evaluate efectiveness of drug therapy or to monitor for the adverse efects of drug therapy in a patient who has not had a recurrence or progression of disease. Patient Care: Management Clinical Interventions/Treatment Knows most appropriate management of selected conditions, including recognizing use/misuse of medications, illicit drugs, or alcohol. Knows immediate management or priority in management, specifcally in emergency or acute cases. This objective is most appropriate in life-threatening emergencies or cases of potential organ failure. Knows most appropriate follow-up or monitoring approach regarding the management plan. Evaluates severity of patient condition in terms of need for referral for surgical treatments/procedures versus other nonsurgical options. Knows appropriate nonhospital health care settings, such as a nursing care facility, hospice care, or at-home care with assistance of health aide. Knows components of rehabilitation program, such as prostheses, psychosocial factors, or motor dysfunction. Educates patient or family regarding self-care, such as breast-feeding, or at-home blood pressure measurement and glucose monitoring. Patient Care: Management Selecting Clinical Interventions (Mixed Management) Selects most appropriate option from set of mixed management options. Patient Care: Management Monitoring/Surveillance for Disease Recurrence or Progression Knows the indications for surveillance for recurrence or progression of disease following treatment. Knows how to monitor a chronic disease in a stable patient where a change in patient status might indicate a need to change therapy. Knows most appropriate long-term treatment or management goals, including continued treatment of a known pa tient. Professionalism and Legal/Ethical Issues Knows the guidelines for obtaining informed consent for treatment including those for children and adolescents, third-party permission, and emergent situations. Knows appropriate prescriptive practices; knows appropriate use of opioids in terminally ill patients. Knows guidelines for reporting fndings to proper authorities, such as social services, police medical society, or coro ner. Recognizes and optimizes human and environmental factors such as workplace design, standardization, and processes. Understands and can apply principles of study design/faws, such as bias and confounding, and methods to address these faws; understands and can apply statistical principles. Understands use and interpretation of statistical principles and measures of association. Compared with, which of the following is the relative risk for in According to these results, how many patients would need to be treated with the new drug to prevent mortality in one patient Makes decisions about patient care based on results of studies or other written materials. Entrapment phenomena occur typically at four different Disorders of the brachial plexus e121 sites giving rise to four different mechanisms (see Chapter 2): Traumatic disorders. An early Lesions at the proximal and middle part of the symptom is paraesthesia with multisegmental distribution. The function of the nerve form a strand that ascends parallel to the spinal cord and enters becomes impaired either as the result of an entrapment the skull through the foramen magnum. Mononeuropathy of the spinal accessory nerve the patient initially complains of intermittent pain in the shoulder girdle area, which soon may become permanent. The fbres Inspection elicits an asymmetrical neckline with drooping originating from the nucleus ambiguus then join the vagus of the effected shoulder. Resisted external rotation of the arm makes the scapula more promi Disorders nent medially. Idiopathic spinal pressure at the medial border of the inferior scapular angle accessory neuropathy may occur in isolation or in combination (Fig. In neuritis of the accessory nerve, the scapula on the with a disorder of other nerves (glossopharyngeal, vagus, long affected side can easily be pushed away at the side. The posterior cord forms a branch that divides Anatomy into two separate nerves: the radial nerve and the axillary nerve. Several interconnections lead to the formation of plexus, either from its supraclavicular or its infraclavicular part. The dorsal nerve (innervating the latissimus dorsi muscle); the superior trunk is created by the fusion of the ventral rami of suprascapular nerve (innervating the supraspinatus and infra C5 and C6. The anterior parts From the infraclavicular part of the plexus the following form the other cords: the superior trunk continues in the nerves originate: the medial cutaneous nerve of the arm (sup lateral cord and the inferior trunk in the medial cord. The cords are lateral, posterior and medial according to their relation to the subclavian/axillary artery. The lateral cord is formed from fbres of the superior trunk, together with fbres Innervation from the middle trunk. The medial the brachial plexus is responsible for the complete motor and cord is the continuation of the inferior trunk. Although it is generally accepted that the aetiology is trauma, the serratus anterior and rhomboid muscles remain compression of the plexus and vascular bundle in the thoracic unaffected. There is slight weakness of the deltoid and supra outlet, different opinions exist about the pathogenesis. The lesion affects the the thoracic outlet is the space bounded by the upper part of C8 and T1 segments, and quite often also C7. Table 1 Affected nerves and muscles in a palsy of the upper part It forms the communicating area at the base of the neck for of the brachial plexus the passage of blood vessels and nerves from mediastinum and neck to the axilla and into which the dome of the pleura rises Nerve Muscle upward. Behind the muscle, in the posterior groove, both subclavian artery and brachial Axillary Deltoid plexus are found (Fig. Humeral head syndrome Symptoms of neurological disturbances are usually found Costoclavicular syndrome but sometimes only features of vascular compression. Only 5% of them will ever suffer from 1, brachial plexus; 2, scalenus anterior muscle; 3, subclavian artery; 4, subclavian vein; 6 5, rst rib; 2 6, clavicle. A cervical rib sometimes gives rise to a palpable It may further lead to a poststenotic dilation, sometimes to mass at the base of the neck. On clinical examination, atrophy of the hypothenar (T1) or There are two types, depending on the clinical features. Acute onset Once a cervical rib has started to interfere with a nerve, the this is unusual, but the diagnosis is important although diff compression does not resolve. Frequently the patient is admitted to the hospital continuously present and tend to increase. All such features draw attention to serious vis Compression of the subclavian artery (Fig. This situation resolves after the arm has been hanging down for a while, the hand may turn a few hours, so that by the time investigations, such as elec white and cold over a period of hours. Paraesthesia may be felt in all digits but may predominate in the median or ulnar distribution. The symptoms disappear after a few minutes, allowing sleep to be continued, although recurrence may take place in the early morning hours. Augmenting the pressure by carrying a heavy object may exceptionally provoke the symptoms as well, but normally only to a mild degree. Cyriax explained this pattern as being the consequence of a diminishing tone in the shoulder muscles, starting in middle age. As a result, the shoulder girdle droops down during the day, resulting in compression of the most medial trunks of the brachial plexus, between the frst rib and clavicle. The process seldom leads to damage of the nerve parenchyma with subse quent muscular atrophy because the brachial plexus can recover every night when the pressure is released. This type of characteristic history should always be followed up with the following additional tests. Sustained elevation of the shoulders the patient sits in a comfortable position and is asked to shrug the shoulders for about 3 minutes (Fig. This causes maximum release of pressure and therefore may bring on the pins and needles and abolish vascular symptoms if present. In thoracic outlet syndrome, the passive movements of the neck are painless and of full range.
The effect of oxygen on respiration and sleep in patients with congestive heart failure arrhythmia journal articles cheap 240 mg calan overnight delivery. Effects of nasal O2 on sleep-related disordered breathing in ambulatory patients with stable heart failure hypertension headache purchase 240mg calan with visa. Nocturnal continuous positive airway pressure improves ventilatory efficiency during exercise in patients with chronic heart failure normal blood pressure chart uk purchase calan without a prescription. Effect of continuous positive airway pressure on mitral regurgitant fraction and atrial natriuretic peptide in patients with heart failure arteria thoracica lateralis proven 240 mg calan. Beneficial effect of bilevel positive airway pressure on left ventricular function in ambulatory patients with idiopathic dilated cardiomyopathy and central sleep apnea-hypopnea: a preliminary study hypertension 55 years discount 240 mg calan with amex. Bi-level positive airway pressure ventilation for treating heart failure with central sleep apnea that is unresponsive to continuous positive airway pressure blood pressure medication spironolactone side effects purchase discount calan line. Effects of dynamic bilevel positive airway pressure support on central sleep apnea in men with heart failure. Effect of oxygen versus adaptive pressure support servo-ventilation in patients with central sleep apnoea-Cheyne Stokes respiration and congestive heart failure. Long-term auto servo-ventilation or constant positive pressure in heart failure and co-existing central with obstructive sleep apnea. Trilevel adaptive servoventilation for the treatment of central and mixed sleep apnea in chronic heart failure patients. Adaptive servo-ventilation in heart failure patients with sleep apnea: a real world study. Beneficial effects of adaptive servo ventilation in patients with chronic heart failure. Comparison of acute and chronic impact of adaptive servo-ventilation on left chamber geometry and function in patients with chronic heart failure. Adaptive servoventilation for treatment of sleep-disordered breathing in heart failure: a systematic review and meta-analysis. Auto-servoventilation in heart failure with sleep apnoea: a randomised controlled trial. Adaptive servo-ventilation in cardiac function and neurohormonal status in patients with heart failure and central sleep apnea nonresponsive to continuous positive airway pressure. Safety and efficacy of adaptive servo-ventilation in patients with severe systolic heart failure. Effect of adaptive servoventilation on muscle sympathetic nerve activity in patients with chronic heart failure and central sleep apnea. Adaptive servo-ventilation therapy improves cardiac sympathetic nerve activity in patients with heart failure. Suppressive effects of adaptive servo-ventilation on ventricular premature complexes with attenuation of sympathetic nervous activity in heart failure patients with sleep-disordered breathing. Impact of adaptive servo-ventilation on cardiovascular function and prognosis in heart failure patients with preserved left ventricular ejection fraction and sleep-disordered breathing. Effects of auto-servo ventilation on patients with sleep-disordered breathing, stable systolic heart failure and concomitant diastolic dysfunction: subanalysis of a randomized controlled trial. Central periodic breathing during sleep in 74 patients with acute ischemic stroke neurogenic and cardiogenic factors. Does hormonal control obviate positive airway pressure therapy in acromegaly with sleep-disordered breathing Effect of octreotide, a somatostatin analog, on sleep apnea in patients with acromegaly. Central sleep apnea is associated with increased ventilatory response to carbon dioxide and hypersecretion of growth hormone in patients with acromegaly. Sleep-disordered breathing, glucose intolerance, and insulin resistance: the Sleep Heart Health Study. Sleep-disordered breathing in nonobese diabetic subjects with autonomic neuropathy. Rostral overnight fluid shift in end-stage renal disease: relationship with obstructive sleep apnea. Relationship of pharyngeal water content and jugular volume with severity of obstructive sleep apnea in renal failure. Decreased chemosensitivity and improvement of sleep apnea by nocturnal hemodialysis. Improvement of sleep apnea in patients with chronic renal failure who undergo nocturnal hemodialysis. Sleep apnea incidence in maintenance hemodialysis patients: influence of dialysate buffer. Adaptive servoventilation improves cardiorenal function and prognosis in heart failure patients with chronic kidney disease and sleep-disordered breathing. Study of oxygen saturation, breathing pattern and arrhythmias in patients of interstitial lung disease during sleep. Sleep quality and associated daytime consequences in patients with idiopathic pulmonary fibrosis. Ventilation and gas exchange during sleep in patients with interstitial lung disease. How common is sleep-disordered breathing in patients with idiopathic pulmonary fibrosis Disordered breathing during sleep and exercise in idiopathic pulmonary fibrosis and the role of biomarkers. Elevated nocturnal desaturation index predicts mortality in interstitial lung disease. A survey of nocturnal hypoxaemia and health related quality of life in patients with cryptogenic fibrosing alveolitis. Oxygen desaturation during sleep and exercise in patients with interstitial lung disease. Does the abnormal pattern of breathing in patients with interstitial lung disease persist in deep, non-rapid eye movement sleep Effect of oxygen on sleep and breathing in patients with interstitial lung disease at moderate altitude. Effect of nocturnal oxygen and acetazolamide on exercise performance in patients with pre-capillary pulmonary hypertension and sleep-disturbed breathing: randomized, double-blind, cross-over trial. The significance and outcome of continuous positive airway pressure-related central sleep apnea during split-night sleep studies. Central sleep apnea on commencement of continuous positive airway pressure in patients with a primary diagnosis of obstructive sleep apnea-hypopnea. Increased propensity for central apnea in patients with obstructive sleep apnea: effect of nasal continuous positive airway pressure. The complex sleep apnea resolution study: a prospective randomized controlled trial of continuous positive airway pressure versus adaptive servoventilation therapy. Interaction of hyperventilation and arousal in the pathogenesis of idiopathic central sleep apnea. Mild-to-moderate obesity: implications for respiratory mechanics at rest and during exercise in young men. Expiratory flow limitation and intrinsic positive end-expiratory pressure in obesity. Oral airway resistance during wakefulness in eucapnic and hypercapnic sleep apnea syndrome. Fat accumulation, leptin, and hypercapnia in obstructive sleep apnea-hypopnea syndrome. Early treatment with noninvasive positive pressure ventilation prolongs survival in Amyotrophic Lateral Sclerosis patients with nocturnal respiratory insufficiency. Lung function accurately predicts hypercapnia in patients with Duchenne muscular dystrophy. Impact of nasal ventilation on survival in hypercapnic Duchenne muscular dystrophy. A comparison of invasive versus noninvasive full-time mechanical ventilation in Duchenne muscular dystrophy. Twenty-four hour noninvasive ventilation in Duchenne muscular dystrophy: a safe alternative to tracheostomy. Relationship between chronic hypercapnia and inspiratory-muscle weakness in myotonic dystrophy. Predictors of need for noninvasive ventilation during respiratory tract infections in medically stable, non-ventilated subjects with amyotrophic lateral sclerosis. A comparison of maximal inspiratory pressure and forced vital capacity as potential criteria for initiating non-invasive ventilation in amyotrophic lateral sclerosis. Effects of non-invasive ventilation on survival and quality of life in patients with amyotrophic lateral sclerosis: a randomised controlled trial. Prognostic value of efficiently correcting nocturnal desaturations after one month of non-invasive ventilation in amyotrophic lateral sclerosis: a retrospective monocentre observational cohort study. Predictors of noninvasive ventilation tolerance in patients with amyotrophic lateral sclerosis. Tracheostomy mechanical ventilation in patients with amyotrophic lateral sclerosis: clinical features and survival analysis. Diaphragm pacing and noninvasive respiratory management of amyotrophic lateral sclerosis/motor neuron disease. Longitudinal effects of noninvasive positive-pressure ventilation in patients with amyotrophic lateral sclerosis. Neuromuscular ventilatory insufficiency: effect of home mechanical ventilator use v oxygen therapy on pneumonia and hospitalization rates. Noninvasive ventilation improves sleep in amyotrophic lateral sclerosis: a prospective polysomnographic study. Percutaneous nocturnal oximetry in amyotrophic lateral sclerosis: periodic desaturation. Effects of non-invasive ventilation on objective sleep and nocturnal respiration in patients with amyotrophic lateral sclerosis. French Multicentre Cooperative Group on Home Mechanical Ventilation Assistance in Duchenne de Boulogne Muscular Dystrophy. Long-term benefits of deflazacort treatment for boys with Duchenne muscular dystrophy in their second decade. Recombinant human acid -glucosidase: major clinical benefits in infantile-onset Pompe disease. Clinical outcomes after long-term treatment with alglucosidase alfa in infants and children with advanced Pompe disease. Long-term effects of nasal intermittent positive-pressure ventilation on pulmonary function and sleep architecture in patients with neuromuscular diseases. Air leaking through the mouth during nocturnal nasal ventilation: effect on sleep quality. Randomised trial of inpatient versus outpatient initiation of home mechanical ventilation in patients with nocturnal hypoventilation. Efficacy and comfort of volume-guaranteed pressure support in patients with chronic ventilatory failure of neuromuscular origin.
Therefore the application of the convex-concave rule to treatment may need to be further informed by the direct method of assessing a restriction of joint gliding blood pressure chart wiki quality calan 240mg. To reflect that change blood pressure normal low purchase calan with american express, the axis (or center) of rotation is called the instantaneous axis (or center) of rotation arrhythmia list buy calan 240mg. Cartilage degeneration often accompanies the presence of a nonfixed axis of rotation blood pressure medication diabetes discount 80 mg calan. An absolute angle is the angle that the distal point of a segment (eg blood pressure pills kidneys purchase generic calan pills, foot blood pressure readings low order calan 80mg overnight delivery, shank, thigh) makes with respect to some reference line (such as the horizontal for sagittal plane movements). A relative angle is the joint angle made by two segments (eg, the knee angle is the angle between the shank and thigh). Relative angles can be stated as either internal (included) or external (anatomic) angles. An internal angle is the angle between the longitudinal axes of the two segments comprisinga joint, while the external angle is the angular displacement from the anatomic position. For example, in the anatomic position, the internal knee angle is 180 degrees, while the external angle is 0 degrees. If this angle were decreased by 30 degrees, the internal angle would be 150 degrees and the external angle would be 30 degrees. It is important to understand the distinction between these three measures and to be consistent in their use. In observational gait analysis, for example, ankle and knee measures are usually external relative angles, while the thigh is usually an absolute angle with respect to the vertical; many motion capture systems, on the other hand, report internal angles for all three joints. Because of the confusion this discrepancy can cause, it is prudent to understand how these terms are being used by various authors and not to assume that there are unambiguous and universally accepted definitions. A force will have a tendency to rotate a body according to its magnitude, its direction, and the perpendicular distance between its line of application and the axis of rotation (this perpendicular distance is known as the moment arm). Knowing that the moment is the product of the force and the moment arm, the length of the moment arm can be manipulated to increase or decrease the force required to complete a task. For example, low back injury prevention strategies are based on the premise of decreasing the moment about the low back during lifting by keeping the load as close to the spine as possible, thus reducing the moment arm of the external resistance. Similarly, flexing the elbows during abduction will decrease the moment arm about the shoulder, thus making the movement easier to perform. On the other hand, during manual muscle testing, the therapist can increase the demand on a muscle by applying the resistance as far from the axis of rotation as possible. Just as forces can be combined together to determine a resultant, they can also be broken into components. The components are useful in identifying the different effects of a force on a joint. For example, a muscle force can be divided into the component that is perpendicular to the bone (causing it to rotate and create a shear force across a joint) and the component that is parallel to the bone (usually increasing the compressive force across a joint). Therefore in addition to causing movement at a joint, all muscle forces will affect the amount of compression at a joint. During rehabilitation of certain joint pathologies, it may be necessary to identify which therapeutic exercises will increase the force of a muscle (to strengthen it) without applying excessive compressive forces across the joint. For example, performing unilateral (as opposed to bilateral) exercises for the lumbar extensors will decrease compressive forces on the spine while increasing the demand on those muscles. Over the range of motion of a joint, the magnitudes of moment arms and forces may vary. The amount of force a muscle can produce is influenced by several properties, including the length-tension relationship, which states that when a muscle is too stretched or too shortened it cannot actively produce as high amounts of force as it can when the muscle is at its optimal length. For example, when using the deltoid to abduct the shoulder from 0 to 180 degrees, the moment arm of the deltoid increases and the force-producing capabilities also increase to a position of optimal length and then decrease. These variations result in an initial increase of torque production, until the optimal position is reached, and then a relatively constant amount of torque production from the deltoids ensues for the remainder range of motion. Based on this, it is important to keep the same manual muscle testing position, especially if the therapist wants to compare among patients or examine the effect of training over a period of time. Tendon-transfer surgeries will often make use of this fact when a certain muscle group is paralyzed. For example, the piriformis is an external rotator when the hip is in a neutral position but becomes an internal rotator when the hip is flexed beyond 90 degrees. When a study refers to a net joint moment, what does that mean and what are the assumptions behind it One of the greatest limitations in biomechanics is that we cannot, with current technology, measure muscle forces in a noninvasive way. Studies will normally report internal moments (as described previously) or external moments (which are as a result of external forces and inertia). Internal moments are equal in magnitude and opposite in direction to the external moment. Joint stability is the ability of a joint to maintain a posture or trajectory similar to an undisturbed behavior in the presence of a perturbation. Joint hypermobility describes a laxity of the joint, where there is increased flexibility and range of motion, and is often used interchangeably with instability by clinicians. However, a hypermobile joint may still be stable because of muscular influence and motor coordination, whereas an unstable joint may not be lax because of neurologic and muscular control. Measures of strength typically determine the maximum force a muscle or muscle group can produce. Skeletal musclesare requiredto produce force, reduce(or absorb) force, or stabilize againsta force. The eccentric muscle action reduces the external force, and consequently decreases the acceleration caused by it. Examining this relationship reveals that greater force can be produced isometrically (when the velocity is zero) than can be produced concentrically, and greater force can be produced eccentrically than can be produced isometrically. Peak eccentric force is estimated to be between 120% and 140% of peak concentric force. Additionally, there is a negative relationship between force and velocity in the concentric range and a positive one between force and velocity in the eccentric range. Yes; mechanical power is the product of the net joint moment and the angular velocity. Although energy can be absorbed by all of the tissues of the body (eg, bone, ligament, muscle-tendon), the muscle-tendon complex has the greatest potential to safely absorb or distribute energy within the body. Eccentric muscle actions are the primary means by which energy is safely absorbed by the body. The amount of force or tension that a muscle can produce varies with the length of the muscle at the time of contraction. When the fibers shorten beyond resting length, the force production decreases slowly at first and then rapidly. This relationship can be used to help explain why surgically lengthened muscles are weak postoperatively (see figure). Although muscles typically do not operate over the entire length, this relationship helps explain the positions used for manual muscle tests, particularly for biarticular muscles. The subsequent concentric action is more forceful than it typically is because it was proceeded by the rapid eccentric action. Plyometric exercises are usually used to improve utilization of the stretch-shortening cycle. A better measure would be stress (force per unit area), which gives an indication of how that force is distributed. Although the term stress is used for reference to internal forces and pressure is used for external forces, clinically they can be used synonymously without much difficulty. Although a certain amount of stress is desirable, too much is believed to be the cause of injury and pain. Patellofemoral pain syndrome is believed to be the result of too much force (from the quadriceps) over too little area (patellofemoral contact area). The smaller contact area seems to have a stronger relationship to symptoms than does the increased amount of force. The insensate and poorly vascularized foot, in association with connective tissue changes, is vulnerable to increases in pressure and consequently the development of pressure sores. If the body weight transmitted to the foot can be dispersed over a larger surface area of the foot, the magnitude of pressure is decreased as is the chance for ulceration. The same factors apply to a person confined to prolonged bed rest; pressure sores may develop on areas where bony prominences contact the bed. The tissue response to a force (or load) is deformation, which is a change in the size or shape of the tissue. Laboratory experiments usually apply a given force (N) to a tissue of known cross-sectional area (mm2) and specified length (mm), in which the resulting deformation (mm) is measured. In vivo, force, either exerted by subject (active) or caused by an apparatus (passive), is measured using a dynamometer and the deformation (here displacement) is measured using an imaging technique (ie, ultrasound). Not all tissues can be measured inthis way; musculotendinousunits are accessibleto testingin vivo, but cartilage is not. Plotting force on the vertical axis and the corresponding deformation on the horizontal axis produces a force-deformation curve, which graphically represents the relationship between the two (see figure). Plastic Region Toe Elastic Region Region Ultimate Strength Yield Point Deformation Force-deformation curve. Depending on the tissue and its role, tissues respond quite differently, and this difference in response is called anisotropism. For example, a tendon responds well to tension, but not as well to shear, and not at all to compression. Human bone can handle compressive force best (such as pushing both ends of the bone toward each other), followed by tension (such as pulling both ends of the bone away from each other), and then shear force (such as pushing the top of the bone to the right and the bottom of the bone to the left). A bending force basically subjects one side of the bone to compression, while the other side experiences tension; therefore the side subjected to tension usually fails first (immature bone may fail in compression first). For torsional loading (such as twisting the top part of the bone, while holding the bottom of the bone in a fixed position), fracture patterns typically show that the bone fails as a result of shear forces and then tension. When the force is applied to the tissue externally, does the tissue return to its original state after the force is removed At lower levels of force the tissue returns to its original form, and therefore this stage is called the elastic region. The yield point is where the material changes from the elastic range to the plastic range. Beyond this yield point, permanent deformation will occur even after the load is removed. The force-deformation curve can be appreciated clinically most easily during ligamentous testing. If the injurious force did not exceed the yield point, the ligament would return to its original length with no detectable changes in joint laxity. If the injurious force exceeded the yield point but did not reach the ultimate strength of the ligament, the ligament would experience a permanent deformation that would be manifested as an increase in joint laxity. If the injurious force exceeded the ultimate strength of the ligament, the ligament would catastrophically fail, and the subsequent force applied during ligamentous testing would be met with no resistance. Discuss some factors that affect the biomechanical properties of tendons and ligaments. There are morphologic, biomechanical, metabolic, and histologic differences between types of cartilage in the joints of the lower extremities. Those differences, in part, are the reason why osteoarthritis is more prominent in the knee and hip joints than in the ankle joint. An obvious example would be the difference in change in volume response to resistive exercise by a muscle and a tendon. A tendon adapts to change more slowly than muscle because it has fewer cells (in this case, tenocytes) that are capable of facilitating adaptation. Evidence on the rate of adaptation of ligaments, cartilage, and intervertebral discs is scarce, but it is believed that they develop more slowly than muscle.
Syndromes
- Have had babies with birth defects in other pregnancies
- Chest x-rays
- Wear long-sleeved shirts and long pants with the cuffs tucked into shoes or socks
- Retinal examination
- Abscess of the brain, skin, spinal cord, or organs such as the kidneys
- Pain that continues after surgery
- Malnutrition and vitamin deficiencies
- Ear discharge or bleeding
- You are a teen or adult with thrush-like sores.
- Loss of ability to interact with other people
Gainesville blood pressure chart order genuine calan online, Fla: Fisheries and Aquatic Sciences Department blood pressure er calan 240 mg on-line, Florida Cooperative Extension Service blood pressure chart old 80 mg calan fast delivery, Institute of Food and Agricultural Sciences blood pressure supplements cheap calan 80 mg on line, University of Florida prehypertension and viagra discount calan 80 mg line, 2007 blood pressure goals jnc 8 cheap 80mg calan with mastercard. If of acceptable quality for fnfsh health, primarily to refer to the killing of animals intended for water in which they have been house or captured human consumption (eg, agricultural harvest, com should be used, and supplemental aeration and temper mercial fsheries) and these Guidelines are not intended ature control may be necessary. If euthanizing a large population any unapproved chemicals for euthanasia prohibits en of fnfsh, it is important to monitor the anesthetic bath try of the fnfsh into the food chain, either by render water quality (temperature, dissolved O, and organic ing, as fsh meal, or as directly consumed product. The euthanasia agent may need With that said, currently there are no drugs approved to be supplemented or replaced periodically. However, there are some ences in anatomy and application seen between fnfsh standard approaches that can be useful for many of the and terrestrial animals (especially with regard to prima more commonly encountered species. Each minimum of 10 minutes and loss of eyeroll (vestibulo method is further classifed as acceptable, acceptable ocular refex, the movement of the eye when the fnfsh with conditions, or unacceptable considering charac is rocked from side to side). The latter is no longer pres teristics of the methods and the environments in which ent in fnfsh that have been deeply anesthetized or eu euthanasia is conducted, including veterinary private thanized. Methods that are acceptable isms, or those with specifc anatomic or physiologic ad with conditions reliably meet the requirements of eutha aptations that prevent use of these indicators, it may be nasia when specifed conditions are met. An unaccept more diffcult to assess loss of consciousness and death, able method does not meet the requirements of euthana and consultation with species experts is recommended. Death possible, products with standardized, known concen usually occurs within 30 minutes. Observers should be advised about the concentrations will be required for euthanasia. These compounds are equivocal or known tion of ketamine, at dosages of 1 to 2 mg/kg, with me carcinogens according to the National Toxicology Pro detomidine, at dosages of 0. Rap Isoeugenol is a potential carcinogen318 so human safety id severance of the head and brain from the spinal cord, in the application of that agent is of concern. Decapitation alone is not con uid anesthetics can be added to water, although they are sidered a humane approach to euthanasia, especially generally not very water soluble. Pithing helps ensure rapid loss of brain water in the container used for euthanizing is helpful in function and death for those species. Doses of > 5 to 20 mL/L (2) Cervical transection using a knife or other can be used (10 times the upper range for anesthesia). Solutions for immersion tween brain and spinal cord) and pithing (destruction should be prepared in concentrations $ 100 mg/L. Well-insulated priate-sized club) can cause immediate unconscious containers, such as coolers, will assist in maintaining ness and potentially death, but should be followed by the ice slurry and a probe thermometer can be used to pithing to ensure death. This pro carp, koi, goldfsh, or other species that can survive at cedure requires training and monitoring for profciency. It is appropriate for zebrafsh and other Anatomic features, such as the location of the eyes, can small-bodied (3. This is a method usually applied to large fnfsh can also be acceptable for small to medium-sized (2. When applied correctly, as secondary euthanasia methods are applied after fn using a well-maintained macerator specifcally de fsh are rendered nonresponsive. Adult zebrafsh should be acceptable or acceptable-with-conditions, frst-step exposed for a minimum of 10 minutes and fry 4 to 7 method. If necessary to ensure death, rapid chilling for dpf for at least 20 minutes following loss of operculum specifed groups may be followed by either an approved movement. Use of a dilute sodium hypochlorite or calci sia methods for zebrafsh embryos < 3 dpf. To ensure um hypochlorite solution may be an adjunctive method embryonic lethality these methods should be followed for early life stages of fnfsh, including embryos and with an adjunctive method such as use of diluate sodi larvae. Flushing of fnfsh into sewer, sep Until further research is conducted, rapid chilling is ac tic, or other types of outfow systems is unacceptable for ceptable with conditions for other small-bodied, simi many reasons. Water chemistry and quality may delay larly sized tropical and subtropical stenothermic spe time to death and result in exposure to noxious com cies. For systems in close proximity to and/or con will determine the appropriateness and effectiveness nected to natural waterways, pathogen release or trans of rapid chilling for euthanasia of fnfsh. Based on these 2 factors, it has been suggested that thesia, is also an unacceptable method. Similarly death rapid chilling in water associated with an ice slurry is a by anoxia and dessication after removal from the water suitable killing method for small tropical and subtropi or by anoxia in water; any death due to exposure to caus cal fnfsh species 3. While metomidate has been used for euthanasia of To ensure optimal hypothermal shock (ie, rapid some fnfsh species, its listing in the Index of Legally killing), transfer of fnfsh into ice water must be com Marketed Unapproved New Animal Drugs for Minor pleted as quickly as possible. Full contact with cold water ensures op embryos and larvae, may require higher concentrations timal exposure and rapid chilling of the fnfsh. Tropical aquarium fnfsh are sold at retail pet often value them as companion animals and share a shops and fnfsh stores from systems housing one or human-animal bond similar to that seen between cli more species of fnfsh per tank. Therefore, populations of fnfsh may become injured or diseased it is important to consider the perception of the client and require euthanasia. Clients should this environment need to be applicable to individual be offered the opportunity to be present during eutha fnfsh, to all fnfsh in an aquarium, to fnfsh held in nasia whenever feasible; however, clients also should be multiple aquariums on a central fltration system, or for educated as to what method will be used and what they fnfsh kept in ponds. For example, clients may not be feasible and depopulation methods may be may believe the excitement phase of anesthesia, which required. Owners should be advised applied blunt force trauma as step 1 of a 2-step method, about the possibility of ketamine-induced muscle followed by pithing. Therefore, od may become hyperactive, which can be disconcert unless a veterinarian is available on-site to oversee use ing for staff and owners. The large number of fnfsh, limited boat space, and species should be sought as necessary. Similarly, fsheries biologists may be faced quinaldine sulfate, and 2-phenoxyethanol. Finfsh eu with situations involving numerous fnfsh requiring de thanized with these methods must not enter the food population (eg, invasive species) rather than euthanasia. Fieldwork on fnfsh may also be conducted on a (2) Rapid chilling (hypothermic shock) is accept smaller scale under conditions that make euthanasia able for zebrafsh (D rerio) and Australian river gizzard feasible. Although a gen exposed to this method may exhibit hyperactivity and eral concern for all environments and situations, the appears to be in distress), eugenol, isoeugenol, or clove potential effects of drug residues and proper disposal of oil. Although a general concern for erator designed for the size of fnfsh being euthanized. Decapitation potential carcinogen318 so human safety in the applica alone is not considered a humane form of euthanasia, tion of that agent is of concern. The pared with concentrations of > 70% used for preser rationale for this approach is similar to that for decapi vation), and acts by inhibiting neuronal sodium and tation and pithing, except that the head is still physi calcium channels in molluscs. Other agents for euthanasia, while less common, (6) Rapid chilling (hypothermic shock) in water have been described and may be useful for specifc ap plications. These agents are not acceptable, however, for 222 solution having a concentration > 1 g/L is not a immersion as a single-step procedure, nor as the frst reliable method for killing some fnfsh in early life step of a 2-step procedure. Rapid chilling followed by immersion in a di the second step (adjunctive methods) of a 2-step eu lute sodium hypochlorite or calcium hypochlorite solu thanasia procedure. Pithing requires detailed anatomic tion is acceptable for zebrafsh embryos and larvae as a knowledge of the species in question. These methods 2-step method and is also acceptable with conditions as are not acceptable, however, as a single-step procedure, a 2-step method for destruction of other (nonzebrafsh) nor as the frst step of a 2-step procedure. And, immersion is an effective route of adminis when euthanizing aquatic invertebrates. Recom is diffcult, 2-step euthanasia procedures are often rec mendations regarding use of adjunctive methods (as ommended in which chemical induction of anesthesia, described previously) may also be necessary to guar nonresponsiveness, or presumptive death is followed antee death. Application of the Methods of killing that do not cause rapid death or latter methods by themselves is generally not consid that cause trauma prior to loss of consciousness are not ered to meet the criteria established for euthanasia. Most small ani the nondomestic captive and free-ranging animals mals will fnd security in a dimly lighted, appropriately discussed in the following sections vary substantially bedded and ventilated crate, box, tube, or similar con in their anatomic and physiologic characteristics, na tainer as this simulates a natural tendency to hide from tive environment, behavior, social structure, responses perceived threats. These variations challenge left within typical social groups or familiar surround the application and effectiveness of euthanasia meth ings as long as possible prior to euthanasia to minimize ods for the many different species. For wild animals in captivity, physical and/or For nondomestic captive or free-ranging animals, the chemical restraint is usually required before euthana methods selected will often be situation specifc, as a sia can be performed. In topics) are relevant to disposal of the remains of non travenous administration of drugs is generally diffcult domestic animals, particularly under feld conditions. Chamber deliv Given the complexity of issues that euthanasia of non ery of inhaled agents having little odor, such as sevo domestic animals presents, personnel are encouraged furane, allows for induction of anesthesia in smaller to consult references on anatomy, physiology, natural species with minimal stress. Research physical surroundings, pheromones or odors from is needed to improve the euthanasia options available nearby or previously euthanized animals, and the pres for some taxonomic groups and circumstances. Hu Terrestrial invertebrates play important roles in labora man safety is of utmost importance for all euthanasia tory research, as display animals, and as companions in procedures, and appropriate protocols and equipment the home. Despite their varied roles, limited guidance (including supplies for addressing human injury due is available on appropriate methods by which inverte to animal handling or exposure to immobilizing drugs) brates may be euthanized. Man systems, some of which do not have close corollaries agement can be guided by the physical and social set in familiar vertebrate systems. Of particular concern for amphib of pentobarbital or similar agent, at a dose equivalent ians and reptiles are differences in metabolism and high to that used for other poikilotherm vertebrates (piscine, tolerances to hypoxia, as compared with mammals, that amphibian, or reptilian) on a weight-to-weight basis will limit the effectiveness of methods based on anoxia. Ideally these agents will be injected di addition, consistent access to the vasculature can be rectly into the circulating hemolymph. However, because challenging and, therefore, many conventional meth many invertebrates have an open circulatory system, true ods of euthanasia are less effcacious for these species. In such cases an intracoelomic injection would be ian or reptile is dead, the application of two or more eu warranted unless otherwise contraindicated. Equipment may be required for restraint of some species in some situations (eg, venomous spe S7. Multiple people may be required for larger spe Physical (eg, boiling, freezing, pithing) and chemi cies, and at least one additional person should be avail cal (eg, alcohol, formalin) methods act by destroying able for emergencies. These methods useful in some situations, particularly for venomous or are not considered to be humane as sole methods of large animals where human safety would be compro euthanasia. Death Barbiturates are best administered intravascularly to may not occur even with prolonged exposure. Regardless of the species or taxonomic group, personnel, or other similar reasons, intracoelomic ad death must be verifed prior to terminating the use of ministration is an acceptable route for administration the inhaled agent, or a second, guaranteed lethal proce of barbiturates. Cave anesthesia and subsequent euthanasia, although appli ats include that inhaled anesthetics are most suitable cation of an adjunctive method to ensure death is rec for smaller species, animals may experience an excita ommended. However, size-appropriate equipment and ap toxicity concerns depending on method of disposal of propriately trained personnel are required, violent mus the remains. Based on rodent models, it is likely that this adjunctive method to prevent recovery. Little information is available on the sensory ca pacity of amphibians and reptiles at the egg stage of S7. It has been assumed that destroyed using methods that are acceptable for adult stopping blood supply to the brain by decapitation animals. Consequently, sensitivity to the meaning and val method of restraint or euthanasia for amphibians and ue to caregivers of animals in this kind of setting is im reptiles unless animals are suffciently small (< 4 g)52 portant. This can be addressed, in part, with attention to permit immediate and irreversible death if placed to stewardship, and relief from pain and anxiety prior in liquid N (rapid freezing). These demonstrating pain or distress while hypothermic, gen situations typically require a more direct approach to eralized prohibitions on hypothermia for restraint or limit how much an animal is allowed to suffer. Localized cooling in frogs situations also require a brief explanation to personnel, may reduce nociception, but this localized effect is not where possible, as well as a more complete explanation appropriately applied to the whole body as a part of eu of the choice of method subsequent to completion of thanasia procedures. Preparing staff ahead of time to be cog animals may be justifed under circumstances where nizant of the possibility of these kinds of situations will human safety could be compromised. Following euthanasia, verifcation of death is im Intramuscular administration of opioids is advan portant. Methods that can be used for verifcation of tageous when other routes of administration are not cessation of cardiac function include, but may not be available.
Purchase 240 mg calan mastercard. OMRON EVOLV Tubeless Wireless Upper Arm Blood Pressure Monitor - Quick Start Guide.