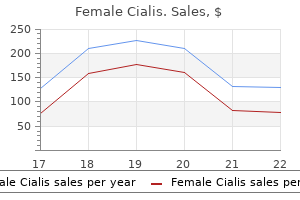
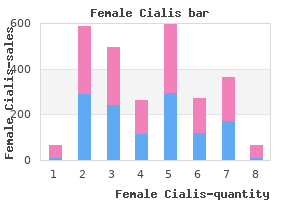
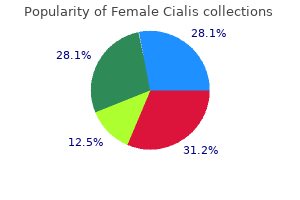
Female Cialis
Dorry Segev, M.D., Ph.D.
- Associate Vice Chair for Research
- Professor of Surgery

https://www.hopkinsmedicine.org/profiles/results/directory/profile/0008001/dorry-segev
Quality Management the quality of care for patients with craniofacial anomalies and related disorders must be carefully monitored by the team providing diagnosis pregnancy 5 weeks 5 days cheap female cialis 10mg free shipping, treatment planning and treatment services women's health center brooklyn purchase female cialis 10mg with mastercard. This requires (1) longitudinal assessments of the outcomes of treatment breast cancer vs prostate cancer buy female cialis 20 mg low price, (2) periodic team review of the clinical outcome data pregnancy on mirena purchase female cialis amex, and (3) team adaptation of treatment procedures when clinical outcome assessments do not reach referenced criteria women's health green coffee cheap female cialis 20 mg without a prescription. Revisions of Clinical Practices the clinical practices presented in this document refect current 26 27 knowledge and experience menstruation queasy stomach purchase female cialis australia. Changes in these practices will be guided by advances in technology and research, including data on clinical outcome. Speech-Language Pathology Orthodontics Cleft Palate-Craniofacial Program American Dental Association Boys Town National Research Hospital Chicago, Illinois Omaha, Nebraska James A. New England Medical Center Orthodontics Boston, Massachusetts Center for Craniofacial Anomalies University of Illinois Nancy C. Smythe (ex-offcio) Chicago, Illinois Executive Director American Cleft Palate-Craniofacial Alphonse R. Parameters for Audiology An Overview Audiology Speech-Language Pathology Cleft Palate-Craniofacial Program Cleft Palate-Craniofacial Center Boys Town National Research Hospital University of Pittsburgh, Pittsburgh, Pennsylvania Omaha, Nebraska Harlan R. Parameters for Otolaryngology Parameters for Plastic and Reconstructive Surgery Otolaryngology Plastic Surgery Cleft Palate and Craniofacial Deformities Institute Cooper Regional Cleft Palate Program St. Medical Sociology Parameters of Care for Pediatrics Craniofacial Center Pediatrics University of North Carolina Craniofacial Team Chapel Hill, North Carolina Loma Linda University Loma Linda, California Timothy A. Surgery Parameters of Nursing Care Oral-Maxillofacial Surgery Nursing Craniofacial Center Cleft Palate-Craniofacial Center University of North Carolina University of Pittsburgh Chapel Hill, North Carolina Pittsburgh, Pennsylvania Katherine Dryland Vig, F. Orthodontics Parameters of Care for Craniofacial Surgery Private Practice Plastic Surgery Oak Park, Illinois Cleft Palate and Craniofacial Deformities Institute St. Louis, Missouri 28 29 Additional Consensus Conference Participants Judy Aguilera-Posen, M. S Speech-Language Pathology Oral-Maxillofacial Surgery Casa Colina Rehabilitation Hospital University of Minnesota Pomona, California Minneapolis, Minnesota Ms. Louis, Missouri Heim Pal Hospital for Sick Children Budapest, Hungary Elisabeth A. AboutFace International Orthodontics Toronto, Ontario, Canada University of Illinois Medical Center Chicago, Illinois Samir E. University of Iowa Plastic Surgery Iowa City, Iowa University of California San Diego, California Philip J. Loma Linda University Medical Center Otolaryngology Loma Linda, California University of Utah Salt Lake City, Utah Sterling K. Mayo Clinic Audiology Rochester, Minnesota University of Pittsburgh Pittsburgh, Pennsylvania Virginia M. Pediatric Dentistry Speech-Language Pathology University of Iowa Univeristy of Iowa Iowa City, Iowa Iowa City, Iowa Patricia A. Speech-Language Pathology Pediatric Genetics Maryland State Health Department University of Nebraska Medical Center Baltimore, Maryland Omaha, Nebraska Ross E. Orthodontics Speech-Language Pathology Lancaster Cleft Palate Clinic Northern Illinois University Lancaster, Pennsylvania DeKalb, Illinois Robert M. Orthodontics Otolaryngology Duke University Medical Center University of Connecticut Durham, North Carolina Farmington, Connecticut David C. Plastic Surgery Plastic Surgery University of North Carolina Seattle, Washington Chapel Hill, North Carolina Judith E. Speech-Language Pathology Speech Science California State University University of Iowa Northridge, California Iowa City, Iowa Duane R. Orthodontics Plastic Surgery University of California University of Chicago San Francisco, California Chicago, Illinois Jerry W. Oral-Maxillofacial Surgery Plastic Surgery Georgetown University Medical Center Rancho Los Amigos Hospital Washington, D. Orthodontics Speech-Language Pathology Academic Center Dentistry Amsterdam Hospital for Sick Children Amsterdam, the Netherlands Toronto, Ontario, Canada Peter Randall, M. Plastic Surgery Oral-Maxillofacial Surgery Hospital of the University of Pennsylvania Baylor University Medical Center Philadelphia, Pennsylvania Dallas, Texas 30 31 Peer Reviewers Marc W. Professional Affairs Division Social Work American Speech-Language-Hearing Association Hughlett L. Genetics Plastic Surgery * Denotes an individual who has a craniofacial anomaly or is the parent of a child with a craniofacial anomaly. This review analyses the literature surrounding the etiology, morphology and clinical anatomy of these kidney fusion anomalies. A systematic literature search was carried out using the Science Direct and Scopus applications. Arterial blood supply was analysed not only basing on Graves pattern, but also a new model of supply created on horseshoe kidneys computed tomography was taken into account. A systematic search of the literature congenital renal fusion anomaly and is characterised by three was carried out using the Science Direct and Scopus morphological anomalies: ectopia, malrotation and changes applications. Jacopo Berengario da Carpi was the first "kidney fusion", "kidney vascular" and "surgery". In total, 41 person to describe this abnormality during autopsies in 1522 articles in journals were refreshed. Finally, 25 references fused at their lower poles by a parenchymal or fibrous isthmus were included in the manuscript. The frequency of appearance is 1 per 400-600 births and occurs more often in men (2:1 ratio). Kidneys ascend from the pelvis to the cidental during routine radiological procedures mesogastrium during the seventh week of fetal development (transabdominal ultrasounds, computed tomography or and reach their final position by the end of the eighth or ninth intravenous pyelography) performed on them for other reasons. Anatomical and clinical aspects of horseshoe kidney: A review of the current literature. Image reproduced with a horseshoe kidney (morphological variant with lateral fusion). Less commonly, the isthmus is situated posterior to those vessels or runs between them. Kidney fusion anomalies show great variation in the origin, number and size of renal vessels, depending on where the ascent terminated during development. The blood supply of the isthmus also has some variability: it may receive blood from the main renal artery, from the abdomi nal aorta (originating above or below the isthmus), the common iliac artery or the inferior mesenteric artery (Mano et al. Considering the embryological aspect, the isthmus blood supply reflects vascular changes of the developing kidneys during the course of kidney ascent from the pelvic to the abdominal position (Raman et al. Ureters usually end in the bladder, but they can Surgical technique includes pyeloureteroplasty, which also be found in an ectopic position (Cascio et al. Treatments are similar to malignancies have a predilection for location in the isthmus, those for a normal kidney. A lower and its multiple arterial blood supplies, is difficult and usually pole approach is taken when possible in a normal kidney needs treatment in an advanced urological centre. Patients with a kidney cortical tumour may be treated often required (Kehagias et al. Stone-free rates (about 80 % after 1 week period) and the percentage of cases with residual fragments were com Horseshoe kidney, due to the location in the lower part parable in both techniques. Complication rates were found to of abdomen and the presence of the isthmus across the midline, be similar in both groups. There are case study reports showing spina bifida and is an important cause of death. Furthermore, association between an anomalous superior vena cava and horseshoe kidney. Horseshoe kidney is associated with an increased relative risk of primary renal carcinoid tumor. Surgical treatment of tumors involving kidneys with fusion pectos anatomicos y clinicos del rinon en herradura: Una revision de anomalies: A contemporary series. Renal autotransplantation after horseshoe kidney injury: a case report and literature review. El estudio puso enfasis especial approach and clinical importance of eleven cases. El suministro de sangre arterial se Imaging of horseshoe kidneys and their complications. Imaging analizo no solo basandose en el patron de Graves, sino que tambien se Radiat. A horseshoe kidney with partial duplex malias congenitas asociadas con el rinon en herradura. Vesicoureteral reflux and ureteropelvic junction obstruction in children Talpallikar, M. Transperitoneal laparoscopic pyelolithotomy versus retrograde intrarenal Medical Faculty University of Rzeszow surgery for treatment of renal pelvis stones in horseshoe kidneys: A Leszka Czarnego 4 35-615 prospective randomized study. Kidney fusion anomalies revisited: clinical and radiological analysis of 209 cases of crossed fused Email: balawender82@gmial. Cardiovascular malformations Received: 06-05-2018 associated with congenital anomalies of the urinary system. Rational: Does the intervention meet the test of competent assessment (diagnosis) and scientifically proven benefit Are known risks and iatrogenic complications weighed against anticipated benefits Cost: Is the monetary cost/reward of the intervention appropriate for the patient, the family, society Therefore, the bass clef [low frequency] is closer to the ear, and the treble clef [high frequency] is more medial. Do you ever require an Eye opener (ie, drink of alcohol) to get going in the morning By being board certifed, physicians show they meet those standards and demonstrate that they have the specialized knowledge and clinical judgment to provide safe, quality patient care. It involves one-year internship training, and a continuing process of professional assessment and learning to support passing an exam improvements in patient care quality, safety, outcomes, and experiences. Afterward, they demonstrate their continuing knowledge by participating in ongoing programs to evaluate and assess their practice. Geriatric Medicine Board certifcation is frst awarded to candidates Dermatology Hematology Subspecialties who meet the requirements in a specialized feld Hospice and Palliative Medicine Dermatopathology of medical practice. Contact the particular board Infectious Disease to confrm all requirements for achieving and Micrographic Dermatologic Surgery Interventional Cardiology maintaining certifcation. The anesthesiologist also diagnoses and treats acute, chronic, disease, organ transplantation, or malignancies of the immune system. However, formal special pathways are available for physicians seeking Specialty training required prior to certifcation: Four years dual certifcation in Allergy/Immunology and Pediatric Pulmonology; Allergy and Immunology and Pediatric Rheumatology; and Allergy and Subspecialties Immunology and Adult Rheumatology. Additional information is available Certifcation in one of the following subspecialties requires additional from the board. Specialty training required prior to certifcation: Prior certifcation in Critical Care Medicine Internal Medicine or Pediatrics; two years in Allergy and Immunology. An anesthesiologist who specializes in Critical Care Medicine diagnoses and treats patients with critical illnesses or injuries, particularly trauma victims and patients with multiple organ dysfunction who require care over a period of hours, days, or weeks. Hospice and Palliative Medicine An anesthesiologist who specializes in Hospice and Palliative Medicine provides care to prevent and relieve the suffering experienced by patients with life-limiting illnesses. This specialist works with an interdisciplinary hospice or palliative care team to maximize quality of life while addressing the physical, psychological, social, and spiritual needs of both patient and family. Pediatric Anesthesiology An anesthesiologist who specializes in Pediatric Anesthesiology provides Colon and Rectal Surgery anesthesia for neonates, infants, children, and adolescents undergoing surgical, diagnostic, or therapeutic procedures as well as appropriate A colon and rectal surgeon diagnoses and treats various diseases of pre and post-operative care, advanced life support, and acute pain the small intestine, colon, rectum, anal canal, and perianal area including management. They treat conditions such Sleep Medicine as hemorrhoids, fssures (painful tears in the anal lining), abscesses and An anesthesiologist who specializes in Sleep Medicine has expertise fstulaes (infections located around the anus and rectum). They also in the diagnosis and management of clinical conditions that occur diagnose and treat problems of the intestine and colon such as cancer, during sleep, that disturb sleep, or that are affected by disturbances polyps (precancerous growths), and infammatory conditions. This specialist is skilled in the analysis and interpretation of comprehensive polysomnography, and well versed in Specialty training required prior to certifcation: Prior certifcation in emerging research and management of a sleep laboratory. This Specialty training required prior to certifcation: Four years specialist provides immediate recognition, evaluation, care, stabilization, and disposition of a generally diversifed population of adult and Subspecialties pediatric patients in response to acute illness and injury. Certifcation in one of the following subspecialties requires additional Specialty training required prior to certifcation:Three to four years training and assessment as specifed by the board. Subspecialties Dermatopathology A dermatopathologist is expert in diagnosing and monitoring diseases of Certifcation in one of the following subspecialties requires additional the skin, including infectious, immunologic, degenerative, and neoplastic training and assessment as specifed by the board. This entails the examination and interpretation of specially prepared tissue sections, cellular scrapings, and smears of skin lesions Anesthesiology Critical Care Medicine by means of light microscopy, electron microscopy, and fuorescence An emergency medicine physician who specializes in Critical Care microscopy.
This is characterized by protrusion Gastroschisis +++ +++ ++ of intracranial structures through a cranial bone Bilateral renal + +++ defect menstrual underpants female cialis 20mg sale. Sonographic Posterior urethral +++ ++ ++ diagnosis is based on the recognition of a cystic valves (meningocele) (Figure 1 womens health 2014 order female cialis 10 mg mastercard. Another malformation that not possible; +++: more common; ++: average; confdently may be diagnosed in the frst trimester is +: less common;: extremely rare menopause panic attacks purchase female cialis without a prescription. Most of the skull pregnancy news cheap female cialis 10 mg on line, and in of alobar and semilobar holoprosencephaly womens health recipes generic female cialis 20mg without prescription, can be particular parietal and occipital bones menopause webmd generic female cialis 20mg with mastercard, are identif reliably detected. The transverse view of the head will able as echoic calcifed structures from 11 completed not show the typical butterfy sign (Figure 1. Therefore, it is possible to assess quite clearly but the fusion of the brain midline structures and of the skull shape and profle between 11 and 14 weeks. It is possible to visualize at appearance during the frst trimester cannot exclude 11 to 13 weeks and 6 days, three spaces within the open spina bifda, because the defect would not be posterior fossa, between the sphenoid and the occip suffciently evident at this stage. However, it obliteration and disappearance of the intracranial should be kept in mind that, in this case, the diag translucency/fourth ventricle, and the enlargement nostic suspicion should be subsequently confrmed of the anechoic space representing the brain stem by a later scan, usually beyond 18 weeks of gestation. According to the most recent lit As mentioned above, in the case of spina bifda, erature [48], it could be useful to measure the ratio the ratio between the brain stem and the fourth ven between the brain stem and the fourth ventricle/ tricle/cisterna magna complex is abnormal (brain cisterna magna complex in cases of suspected spina stem/brain stem-occipital bone diameters ratio is bifda (brain stem/brain stem-occipital bone diame higher in fetuses with open spina bifda than in ters ratio is higher in fetuses with open spina bifda normal fetuses). Ventriculomegaly may ance or measurement of the structures of the poste be secondary to brain destruction (congenital infec rior fossa, the operator could be alerted to accurately tion or a vascular mechanism); malformations; examine the anatomy of the spine, aiming for direct hydrocephalus; neoplasms; or a combination of two visualization of any spinal defects (Figure 1. Development are usually related to a second or third-trimester of the posterior fossa structures is ongoing during ventriculomegaly, rather than a frst-trimester one. In particular, the cerebellar ver the frst trimester, has been reported [14,43,50]. Midsagittal view of the face; trans normal development of the cerebellum is not taken verse view at the level of the orbits and of the upper lip/ into consideration. Even if the correct diagnosis of hard palate; coronal view, to visualize the hard palate these abnormalities cannot be made this early, the and retronasal triangle [51]. The examination of the fetal profle orbits may show the two orbits, symmetric and normal in the midsagittal view of the face may show a chin in size/position. This fnding is arch-shaped calcifed palate and the upper lip above it usually not easily detected, because the size of the should be visualized, without any evident disruption. This fnding should raise suspicions of chromosomal abnormalities (mainly trisomy 18) and genetic syndromes. When diagnosed, a detailed exam ination of the fetal anatomy should be encouraged. The routine examination of the pal ate and lip could lead to an improved detection of facial cleftings. The usually diffcult visualization of the lip and the small dimensions of these struc tures make the diagnosis possible only for the major defects (Figure 1. In selected cases, the transvag inal approach may contribute to improve the detec tion of these defects. Thorax and Heart the thorax, and several basic features of cardiac anat omy, can be evaluated during the frst trimester. The chest normally contains lungs of homogeneous echo genicity on ultrasound, without evidence of cystic or solid masses. Routine examination of some ultrasound markers for chromosomal abnormali ties has recently improved the early detection rates of fetal cardiac anomalies. The lumen of right and left ventricle separated by the interventricular septum can be clearly identifed. This transverse view provides important information on the direction of blood fow in the two arches and on the location and dimension of the aortic arch. In this frst trimester and require further evaluation after a view, the assessment of the cardiac situs and its rela few weeks [13,56]. The four-chamber view Also, an evaluation of the two atrioventricular con could reveal an abnormal position of the heart, due nections by two-dimensional ultrasound and color to compression by bowel loops or stomach or liver fow mapping should be performed; in case of congenital diaphragmatic hernia. The transverse view of the the cases of diaphragmatic hernia had been diag chest, with the examination of the four-chamber nosed in the frst trimester [14] (Figure 1. In order of the abdomen, including the visualization of the to confrm the situs solitus, it is also important to stomach, the outline of the abdominal wall, and cord check whether the fetal stomach is on left side of the insertion. Situs abnormalities could, therefore, already be detected in the frst trimester, if we were to assess Method. The stomach must be shown in a transverse these structures and their position routinely. Color Doppler image at 13 weeks demonstrating, in the fve-chamber view, the ventricular septal defect with an overriding aorta (arrow). However, care should be taken in diagnosing an exomphalos before 12 weeks, because the physiologic herniation of the bowel in the cord completely regresses only at the end of 11 weeks. Therefore, if an exomphalos containing only bowel loops is suspected at this gestational age, it is safer to wait 1 week in order to get a confr mation of the diagnosis. Sometimes, cord loops could give the impression of a bowel hernia tion and the color Doppler could be helpful in the differential diagnosis. It is important to differenti ate between exomphalos and gastroschisis because of the strong association between exomphalos and chromosomal abnormalities, like trisomy 18 and 13 (about half of the cases) [46,57]. The heart (H) is shifted to the right by intra dition could resolve spontaneously, if there is just thoracic viscera. If herniation of the liver is already visi well as the normal size and position within the abdo ble in the frst trimester and the exomphalos does men. The cord insertion can be visualized either in a not resolve spontaneously, surgery is required after transverse view or in a midsagittal one. Gastroschisis is not usually correlated with view, the outline of the abdominal wall can be assessed increased risk for chromosomal abnormalities, but to exclude any abdominal wall defects. Transverse view of the fetal abdomen showing herniation of the liver in the sac (arrows). The kidneys are already visible in nosis is based on two of the three features below: the frst trimester, but they have similar echogenicity exencephaly/cephalocele, abdominal wall defect/ to the surrounding tissue; therefore, visualization is thoracoschisis, and limb defect. The visualization could be improved by num, but no other defects usually are associated. Midsagittal view of a fetus at 13 weeks showing massive dilatation of the bladder, occupying almost all the abdominal cavity. This fnding is cor enough time to allow the bladder to fll up, it is man related with chromosomal abnormalities (mainly datory to clearly visualize the kidneys either trans trisomy 13 and 18) in a signifcant number of cases abdominally or, if necessary, transvaginally. We need to classify at least two different kidneys are not visible, bilateral renal agenesis con types of megacystis, both visible in the frst trimes dition has to be suspected, and a further confrma ter. A bladder diameter more than 15 mm is usually tion could be the impossibility to demonstrate the related to ureteral obstruction (complete urethral renal arteries by color or directional power Doppler valves or urethral atresia) (Figure 1. This advisable to wait until 16 completed weeks, when type of megacystis is strikingly evident at this stage, oligo-anhydramnios develops. View of the hands and feet of the bladder is between 7 and 15 mm, it has been showing the fngers. Basically, the examination of the limbs should is normal, spontaneous resolution of the megacystis aim to show the presence of all three segments of each occurs in about 90% of cases. A closer exam because though the kidneys can be visualized, as pre ination, by dedicated views of the open hands and the viously mentioned, they cannot always be visualized foot soles, could show whether there are fve fngers on as clearly as they ought to be. Ultrasound image showing a fetal arm with a normal humerus and a small forearm characterized by the presence of only one small bone (the ulna). The diagnosis of limb abnormalities is easier when the condition is not isolated, such as in Figure 1. The routine chromosomal abnormalities (trisomy 18) or with early visualization of a midsagittal view of the leg, showing arthrogryposis [62]. The position of the foot in the the normal relationship with the foot (the sole should earlier stages of embryologic development is actually be not visible in this view), could improve the detec intrarotated, making it diffcult to differentiate patho tion of severe talipes, mainly when associated with logical talipes from the positional one [62,63]. In particular, severe oligohydramnios, from premature rupture of membranes or renal anomalies, Maternal causes of impaired acoustic window. The most and severe polyhydramnios, from fetal anomalies, important factor that may greatly reduce the diagnostic twin-to-twin-transfusion syndrome, or idiopathic, can potential of a transabdominal ultrasound examination be responsible for an impairment of the acoustic win is the presence of maternal obesity, which, unfortu dow for different reasons. In oligohydramnios, the nat nately, is becoming a real problem due to the increased ural contrast agent represented by the amniotic fuid is prevalence of this condition in the populations of the absent and, in addition, the limbs are often adducted; developed countries [64]. The impairment of the acous these two factors usually limit assessment of the fetal tic window exhibits a positive linear correlation with the limbs and heart. With severe polyhydramnios, the thickness of the abdominal subcutaneous adipose tissue. Finally, of these anatomic regions are the periumbilical area, the most frustrating condition to be confronted with where there is virtually no adipose tissue and which may in the course of an ultrasound examination is, in our be exploited if no air is left between the transducer and experience, a previous abdominoplasty. In this case, the actual maternal umbilicus, and the lateral regions of several concurrent factors contribute to the limitation of the abdomen. To take advantage of this type of approach, cal wound scar; residual abdominal fat; and a dramatic the patient may be asked to roll onto one side (which increase in abdominal frmness. All represent a frustrat one depends on the position of the fetus) in order to bet ing if not insurmountable problem. Often, using this type of approach, the increased mus Fetal causes of impaired acoustic window. The most cular resistance offered by some patients (see above) also common cause of (fortunately transient) impairment of tends to be reduced. A third preferential point of access the acoustic window is represented by an unfavorable is the suprapubic area/fold. However, in these craniofacial anatomy may be assessed through the peri cases, it is often suffcient to rescan the woman after umbilical area. As a result, the mid-trimester anomaly can be unremarkable in all conditions covered by the former definition [65]. Unfortunately, the clinical use of 3D ultrasound has been in part obstructed by its use (misuse Although this may be partly true in those cases in which a fetal malformation has been detected, though only for some organ systems, as explained in the various chapters, the use of 3D ultrasound in the screening setting so far has not been validated at all. It is possible to to 3D ultrasound, from the volume acquisition proce assess the overall quality of the acquired volume by looking dure to offine navigation and reconstruction. The number of vertical artifacts the currently available techniques and imaging modes, (arrows) corresponds to the number of gross fetal movements. However, an easy and procedures described here relate to the equipment and fast way to assess the quality of an acquired volume technologies developed by this manufacturer. The acquisition of the volume is based on the movement of the array housed inside the Multiplanar imaging. This image modality represents transducer: when the procedure is activated, this array the key approach to the study of fetal anatomy in nor performs a slow single sweep, automatically recording mal and abnormal conditions. This volume consists of a high the three orthogonal planes are displayed (Figure 1. In addition, the quality of the volume is condi surface appearance of a given structure (surface mode). Once the 3D volume is opened, the three orthogonal planes sues, displaying the fetal bones. By moving the small caliper, yellow in (a), red in (b), spine with the occipital bone (Occ) and the scapulae (S) on the blue in (c), it is possible to assess in detail the anatomic structure left and the lower spine with the iliac wings (Sa) on the right. This example illustrates the multiplanar rendering of a normal fetal face at 32 weeks of gestation. This example is (arrows) (Occ: occipital bone; Pa: parietal bones) (b) detailed the same as in Figure 1. In fact, its algorithm inverts the color code increased, and the maximum mode option is activated, assigned to black and white pixels (voxels in 3D). The the soft tissues become transparent and the fetal skele final output is a cast-like image of the studied structure; ton is displayed (Figure 1.
Order female cialis 10 mg free shipping. USF Health Opens New Pamela Muma Women’s Health Center.
Classical prophylactic medication: dexamethasone 8 mg 13 hours women's health clinic yonkers ny cheap female cialis, 7 hours women's health clinic kingswood generic female cialis 20mg amex, 1 hour before the admi nistration of docetaxel; clemastine 1 mg 13 hours menopause effects cheap female cialis 20 mg without prescription, 7 hours menstruation 4 days early purchase female cialis visa, 1 hour women's health exercise plan order female cialis 20 mg with amex, before the administration of docetaxel; followed by dexamethasone 8 mg p womens health institute taos nm buy generic female cialis 20 mg line. Development of a polysorbate 80-free docetaxel formulation (pegylated liposomal docetaxel, doce taxel-fibrinogene-coated olive oil droplets, docetaxel encapsulated nanoparticle-aptane bioconjuga tes, submicronic dispersion formulation). Acral erythrodysesthesia syndrome caused by intravenous infusion of docetaxel in breast cancer. Doxil* (liposomal formulation of doxorubicin coated with polyethylene glycol) is less myelo and cardio-toxic but is characterized by dominant and dose-limiting mucocutaneous reac tions. Hand-foot syndrome or palmo-plantar erythrodyses thesia (frequent, sometimes severe with necrosis). Direct degranulation of mast cells or circulating basophils without antibody mediation. Pegylated liposomal doxorubicin-related palmo-plantar erythrodysesthe sia (hand-foot syndrome). Complement activation following first esposure to pegylated liposomal doxorubicin (Doxil*): possible role in hypersensitivity reactions. S Clinical manifestations Cutaneous: urticaria, pruritus, rash, allergic contact dermatitis, injection-site reactions, alopecia, stomatitis. S Mechanisms One case of anaphylaxis to gelatin included in erythropoietin products. High concentration of polysorbate 80 in the formulation of epoetin alfa leads to micelle formation. Epoetin molecules are integrated into the surface of these micelles, so several epoetin molecules are presented to the immune system in a regular spacial configuration which can trigger the immune system (pure red cell aplasia). Corticosteroids +/ cyclophosphamide; cyclosporine, kidney transplant (pure red cell aplasia). Hypersensitivity reactions to the polysorbate contained in recombinant ery thropoietin and darbepoietin. An allergic reaction to erythropoietin secondary to polysorbate hypersensiti vity. S Diagnostic methods No in vivo or in vitro method is currently available for diagnosis. The role of polysorbate 80 (Tween 80) used as an excipient in the parenteral formulation is doubtful. Continous administration without modification (65% successful) Premedication with antihistamines and/or corticosteroids. Successful treatment with etoposide phosphate in patients with etoposide hypersensitivity. Safe administration of etoposide phosphate after hypersensitivity to intra venous etoposide Br J Cancer 2002;86:12-3. Successful rechallenge with etoposide phosphate after an acute hypersensitivity reaction to etoposide. Hypersensitivity reactions to epidophyllotoxins in children with acute lympho blastic leukemia. S Diagnostic methods Skin tests One case with intradermal test positive (anaphylactic shock). Anti-Ssa/Ro antibody as a risk factor for fluorouracil-induced drug eruption sho wing acral erythema and discoid-lupus-erythematosus-like lesions. Stevens-Johnson syndrome/toxic epidermal necrolysis in a patient receiving concurrent radiation and gemcitabine. Hypersensitivity pneumonitis in advanced non-small-cell lung cancer patients receiving gemcitabine and paclitaxel; report of two cases and a review of the literature. S Diagnostic methods Skin biopsy: epidermal thickening, flattening of the dermoepidermal junction, basal layer degene ration, colloid body formation. S Management Hydroxyurea can be continued if necessary with no worsening of cutaneous lesions. Hydroxyurea-induced hypersensitivity pneumonitis: a case report and lite rature review. Fever caused by hydroxyurea: a report of three cases and review of the literature. S Clinical manifestations Differentiate from non-allergic side effects (headache, gastrointestinal symptoms). S Diagnostic methods Skin tests Prick tests: ondansetron: 2 mg/ml, dolasetron: 20 mg/ml, granisetron: 1 mg/ml. Challenge test: positive S Mechanisms IgE-mediated hypersensitivity in some cases. Ondansetron and tropisetron share an indole heterocycle, ondansetron and granisetron do not, which explains the absence of cross reactivity between these two drugs. Hypersensitivity reactions associated with 5 hydroxytryptamine 3 receptor antagonists: a class effect. Used in the treatment of chronic myeloid leukaemia and malignant gastrointestinal stromal tumors. Others: cutaneous and oral lichenoid induced eruption, pityriasis-rosea-like eruption, vasculitis, cutaneous hypo and de-pigmentation associated with photosensitivity, hyperpigmentation (skin, nails and hair), exacerbation of psoriasis or induced acral psoriasiform hyperkeratosis. S Mechanisms Changes in tyrosine kinase signaling (altered c-Kit affects the development of epidermal inflamma tion). S Management Prednisone 1 mg/kg/day tapered to 20 mg/day over several weeks and gradual reintroduction of imatinib 100mg/day initially increased by 100 mg/week as the prednisone dose is being tapered. Successful progressive challenge after a cutaneous reaction to imatinib mesylate (Gleevec*): a case report and review of the literature. Local reactions (frequent): erythema, erosion, excoriation, edema, desquamation, pruri tus, burning, pain, localized hyperpigmentation or hypopigmentation, infections. Others local reac tions (less frequent): dysuria, localized pemphigus foliaceus, aphthous ulcers after treatment of acti nitis cheilitis, angioedema. Systemic reactions: erythema not strictly localized to the site of applica tion, exacerbation of psoriasis (generalized reaction), exacerbation of eczema. Generalized exacerbation of psoriasis associated with imiquimod cream treatment of super ficial basal cell carcinoma. Aphthous ulcers associated with imiquimod and the treatment of acti nic cheilitis. Vitiligo-like hypopigmentation associated with imiquimod treatment of genital warts. Increased specific IgE antibodies found in patients in whom L-asparaginase infusions are followed by allergic reactions. High titers of IgG3 or IgG4 anti L-asparaginase may predict L-asparaginase allergy. Complement activation induced by formation of immune complexes of L-asparaginase and specific IgM and IgG class antibodies. S Management Avoidance, but hypersensitivity reactions to L-asparaginase do not impact on the remission dura tion in adults and childrens with acute lymphoblastic leukemia. Hypersensitivity reactions to L-asparaginase do not impact on the remis sion duration of adults with acute lymphoblastic leukaemia. Hypersensitivity reactions to Escherichia Coli derived polyethylene glycola ted-asparaginase associated with subsequent immediate skin-test reactivity to E. An open-label multicenter study of polyethyleneglycol-L-asparaginase for the treatment of acute lymphoblastic leukaemia. Dermatologic adverse effects of lenalidomide therapy for amyloido sis and multiple myeloma. Local erythema and pruritus due to irritant reactions, contact delayed hypersensitivity or allergic contact dermatitis (frequent with topical use: more than 50% of treated patients in the first 3 months). Others: erythema multiforme-like dermatitis, bullous reactions, Stevens-Johnson syndrome, xerosis, hyperpigmentation, induced squamous cell carci noma. S Diagnostic methods Skin tests: prick tests and patch tests positive in patients with reactions to topical mechlorethamine. Dilutions of the solution in water: from 10 mg/1200 ml to 10 mg/1800 ml every day for a week. If tolerated, double the dose the following week until a tolerable dilution is reached. Treatment of early-stage mycosis fungoides with twice-weekly applica tions of mechlorethamine and topical corticosteroids. A prospective study of cutaneous intolerance to topical mechlorethamine therapy in patients with cutaneous T-cell lymphomas. Topical desensitization to mechlorethamine (nitrogen mustard) contact hypersensitivity. Stomatitis, erythema and oedema (slight or severe with blistering and pain), localized scleroderma (with isolated limb perfusion with melphalan). S Diagnostic methods Leukocyte migration inhibition test: one positive test in a case of interstitial pneumonitis. S Mechanisms Alkylation reaction may occur in vivo, and altered proteins may serve as new antigens capable of sti mulating antibodies to the hapten-protein complex. Some reactive patients may be switched to oral melphalan with no further reaction. Acute, reversible, interstitial pneumopathy induced by melphalan (Article in French). S Diagnostic methods Skin tests: prick tests, intradermal tests and patch tests are positive in a few cases. Adverse hypersensitivity reactions to mesna as adjunctive therapy fo cyclophos phamide. After cyclophosphamide treatment of patients with systemic lupus erythematosus and dermatomyositis. Positive reaction in one case; com plicated by syndromic reaction (anaphylactic shock). Management of an anaphylactoid reaction to methotrexate with a stepwise graded challenge. Methotrexate-induced papular eruption in patients with rheumatic disease: a distinctive adverse cutaneous reaction produced by methotrexate in patients with collagen vascular diseases. S Incidence Cutaneous side-effects: 9% of patients treated with intravesical instillations. S Diagnostic methods Skin tests Intradermal test: one immediately positive intradermal test reported in a patient with an imme diate reaction. Systemic allergic contact dermatitis from intravesical instillation of the antitumor antibiotic mitomycin. Dermatitis due to intravesical mitomycin C: a delayed-type hypersensiti vity reaction Cutaneous: injection-site reactions: pain, burning, pigmentation (bluish), necrosis (rare), rash, edema, purpura (with thrombocytopenia), discoloration of the nails, stomatitis, alopecia. S Diagnostic methods Skin biopsy: leukocytoclastic vasculitis in a case of erythematous vesicular rash. Others: carcinoma, cutaneous and mucosal infections (viral and mycotic), alopecia. Hypersensitivity to mycophenolate mofetil in systemic lupus erythe matosus: diagnostic measures and successful desensitization. S Clinical manifestations Generally after 7 to 9 cycles, within minutes following infusion initiation. S Management Pretreatment with intravenous calcium gluconate and magnesium sulfate. Pretreatment with dexamethasone or methylprednisolone, dyphenydramine, cimetidine 30 minu tes before oxaliplatin infusion.
If a systemic reaction should occur menstrual flow is actually deteriorating discount female cialis generic, epinephrine There is some evidence that anaphylactoid reactions to may not be totally effective in patients taking blockers women's health clinic in ottawa effective 20mg female cialis, and venom occur in a substantial number of patients with masto epinephrine may adversely affect patients taking monoamine cytosis or urticaria pigmentosa having relatively high consti oxidase inhibitors pregnancy 0-12 weeks discount 20 mg female cialis fast delivery. The late-phase cutaneous response is lin testing may sensitize a small number of individuals to a continuation of either prick/puncture or intracutaneous test penicillin womens health group rocky hill ct purchase 10 mg female cialis. Intracutaneous tests often do not correlate well the late-phase cutaneous reaction develops progressively with serum specific IgE levels menstruation rituals buy cheap female cialis. One possible explanation for at sites of immediate wheal-and-flare reactions and is char this disparity was a recent study in which binding of allergen acterized by erythema menstruation urinalysis order female cialis 20mg overnight delivery, induration or edema, and dysesthe sia. Immediate systemic reactions are occur in the absence of an immediate skin test response and more common with intracutaneous tests; 6 fatalities were may be confused with cell-mediated, delayed hypersensitiv reported in a recent retrospective survey. Prescreening with prick/puncture approximately 36% of children undergoing skin tests for tests is a practical way to avoid life-threatening reactions to suspected allergies. The late-phase cutaneous response tivity (eg, anaphylaxis to foods and drugs) is suspected. Although adverse events occurring after intracutaneous 193,194 Many allergens have been implicated. Large local reactions, both Late-phase cutaneous reactions occur after both immune immediate and late, may cause discomfort and occasionally and nonimmune (eg, 48/80, kallikrein) mast cell activation. Immediate systemic reactions are more com that have induced the late-phase cutaneous response include mon with intracutaneous tests because larger volumes are anti-IgE antibodies and the following allergens or antigens: injected. Six fatalities attributed to intracutaneous skin tests aeroallergens (molds, pollens, danders, mites, and enzymes), were reported by the Committee on Allergen Standardization 205,206 195 penicillin, heparin, insulin, and possibly some foods. Five of these patients had asthma and were the propensity to develop the late-phase cutaneous response tested without preceding prick/puncture tests. No fatalities may be dependent on the type of antigen, host sensitivity, and were associated with intracutaneous testing in the most recent 207 147 the concentration of injected antigen or allergen. To reduce the likelihood of adverse reactions during skin Reading the test results testing, several precautions may be taken. The late-phase cutaneous response prick/puncture test is a practical way to avert an untoward should be read between the 6th and 12th hours after the skin number of adverse local and/or systemic responses in routine tests are applied; measurements of mean diameter and/or area skin testing of patients. Even greater precautions should cutaneous response increases rapidly (doubling or tripling in be observed if patients are suspected of having exquisite size) during the first 2 hours. Further research is needed genic (eg, from Fel d 1) peptides can distinguish between a to clarify this issue. Immunochemical histologic analysis at various indices stages of the inflammatory milieu of a late-phase cutaneous None of these indices are available for late-phase cutaneous response reveals a diversity of cells, including macrophages, response because there are too few clinical trials to provide a eosinophils, neutrophils, tryptase positive mast cells, Lang practical basis for determining sensitivity, specificity, pre erhans cells, and, interestingly, large numbers of ba 210,211 dictability, or likelihood ratios. Possible severe im described in association with the late-phase cutaneous re mediate reactions would only occur during the initial imme sponse. Although the clinical relevance of reading period of intracutaneous testing could possibly persist late-phase cutaneous response is not as yet fully established, or worsen and present a clinical problem if the mediator several randomized, controlled studies suggest that reduction release was intense enough. This could occur at the same time in sizes of late-phase cutaneous response may parallel clinical as the late-phase cutaneous response might be expected to response to immunotherapy. In both safety surveys previously discussed, no evi Although the clinical relevance of late-phase cutaneous dence of life-threatening events or fatalities to late-phase response cannot yet be delineated with certainty, there has cutaneous responses has been reported. Antihistamines may been preliminary progress about some potential clinical ap offer symptomatic relief for persistent erythema and pruritus, plications. At least 4 randomized, controlled clinical trials of presumably due to histamine newly released from previously immunotherapy in patients with allergic rhinitis have shown unstimulated mast cells recruited to the lesion. If inhalation allergy is narrowly confined to a single season (eg, ragweed in North America or birch in European northern Number of Skin Tests countries), a limited number of relevant skin tests would Summary Statement 43. By contrast, perennial symptoms would require a more tions (eg, region of the country), occupation, and activities. Similarly, skin America may prove to be unattainable, expert consensus tests for a few drugs that cause anaphylaxis (eg, penicillin, panels have ventured opinions with the expectation that rel succinylcholine analogs) reliably predict life-threatening ana ative consistency of skin testing, including number of tests, is phylactic reactions. A history of anaphylactic reactions to a desirable goal for both clinical practice and research. There are these opinions are based on current principles regarding 6 commercially available skin test preparations for stinging constitutive allergenicity, cross-allergenicity, aerobiologic and biting insects (eg, honey bee, wasp, yellow jacket, yellow monitoring, and correlation with organ challenge testing or faced hornet, white faced hornet, and imported fire ant). Of these, there is sources should be used to determine whether specific allergen general agreement that significant indoor allergens such as tests based on pretest probability are likely to confirm a house dust mite, prevailing indoor fungal allergens (Penicil suspected clinical diagnosis. Pollens may cutaneous skin tests are important for diagnosis of inhalant also be found indoors when windows are kept open. Some clinicians prefer to initially screen with prick/ geographic variability of airborne-pollinating plants through puncture followed by intracutaneous tests if the results of the out the floristic zones of the world, particularly in North former are negative, whereas others exclusively use intracu America, raises a cogent concern about how to select the taneous tests. Initial prick/puncture screening followed by number of skin tests and treatment reagents for this class of end point intracutaneous serial titration is an accepted regi allergens. Only prick/puncture tests should be performed applicable to the selection process. Each of these situations involves the postulates regarding clinically significant pollen allergens special approaches, which will be addressed in the following originally proposed by Thommen should be satisfied: (1) discussion. For in considerable distances; and (5) the plant producing the pollen dividual patient evaluations, a larger number of skin tests is is widely and abundantly distributed. This applies to such plants as golden Although recognizing that the history may be a relatively rod, daisy, sunflower, dahlia, and rhododendron. Although insensitive predictor of clinical sensitivity in some situations, pine pollen satisfies postulates 2 to 5, it is not a clinically certain historical features serve as important pretest probabil important allergen because its constitutive allergenicity is ity guides to the numerical extent of skin tests. In toddlers, sensitization is more apt to known pollen season, controlled laboratory, or environmental reflect intense and prolonged exposure to allergens encoun exposure unit challenges. Cross-allergenicity among major classes must be sufficiently high to fulfill the other Thommen pos of airborne fungi has not been well delineated. Annual pollen sampling data in various regions of the these facts about cross-allergenicity are particularly ger country are available at the National Allergy Bureau web site mane to formulation of treatment extracts for a particular ( Relatively few foods account for most IgE epitopes with pollen allergens not only from other tree pol 255 mediated allergic reactions in both children and adults. Commer ularly germane to the decision about number of tests because cial fruit and vegetable extracts rapidly lose potency so many it demonstrates clearly that skin test reactivity alone cannot clinicians either prepare fresh extracts of these classes of decide the clinical significance of an allergen. This method is centage of reactions to the ornamental black locust in polli preferred to detect strain differences in fruit allergens (eg, nosis patients is ascribed to cross-sensitization to panaller 126 257 apple). This is termed an allergy 257 potential risks, intracutaneous tests to foods are not recom mirage. The choice and number of test allergens should be melain-type cross-reactive carbohydrate determinants caused continuously refined in accord with scientific advances, bo by timothy grass or mugwort pollen has also been reported in tanic and aerobiologic surveys, demographic trends, and venom sensitization. Practice must be tensive cross-sensitivity among all pollens must be critically directed to the best documented concepts of allergen preva reviewed either when selecting a skin test panel or when lence, geographic distribution, and immunochemical relation interpreting the results. The reported prevalence of outdoor airborne fungi depends Although no prospective studies provide direct evidence on sampling technique (viable vs nonviable; bioaerosol vs for these issues, the literature concerning clinically relevant surface) and the collecting device. This issue had Cladosporium and Alternaria species are predominant in the received serious consideration by the Joint Task Force on summer months. Indoor mold sampling almost always detects Practice Parameters in conjunction with expert consultants species of Aspergillus and Penicillium. Respiratory challenge tests are used 40 intracutaneous tests) for inhalant allergens, as published in when an objective gold standard for establishing clinical the Practice Parameters on Allergy Diagnostic Testing in sensitivity is indicated. However, Historically, provocation challenge tests with inhalant al routine annual tests without a definite clinical indication are lergens have been used to clarify the role of allergens in clearly not indicated. They may occasionally facilitate or confirm Based on recent extensive food allergy research reviewed the diagnosis of clinical sensitivity when the history is sug in Food Allergy: A Practice Parameter, relatively few foods gestive but skin and/or specific IgE test results are nega are responsible for most clinical food allergy suggested by the tive. However, this gen They also are used to evaluate response to therapy, either erality does not exclude the possibility that larger numbers of pharmacologic or immunologic. Tests for venom and drug sensitivities are They are often required to substantiate clinical sensitivity of not included in this calculation because these tests are per occupationally induced diseases after cutaneous and respira formed only in patients with a strongly suggestive history of tory exposure to proven and possible new workplace aller anaphylaxis and not routinely in patients who present with gens. New techniques for assessing local and test allergens may be required for exposures to occupational systemic inflammatory biomarkers are emerging as useful allergens, in patients with unusual hobbies or personal con clinical diagnostic adjuncts for both immediate and delayed tact with less common pets (eg, rodents) or livestock. Conjunctival challenge tests are usu From time to time, patients may present with symptoms ally conducted for suspected localized eye allergy but in some caused by previously unidentified substances that potentially cases they may also be helpful in investigating nasal allergy. There is a role for testing such patients (B) with properly prepared extracts of a new allergen. Conjunctival challenge tests are insufficient evidence, however, to justify tests for nonproven evaluated by symptoms of itching and objective indices, agents, such as newsprint, sugar, cornstarch, orris root, to including tear volume, amount of mucus, and palpebral or bacco smoke, cotton, formaldehyde, and smog. The inferior subsequent overview of this study questioned whether the conjunctival fornix is a point where the inferior palpebral and diagnostic yield of such a strategy was worthwhile. For solutions, a starting concentration is usually 3 may tend to go beyond the nasal passages into the lower to 4-log fold less than prick/puncture allergen concentrations airways and produce undesirable effects. If test results are negative at these dilu soaked with fluid appear to provide the most localized deliv tions, serial log fold increasing concentrations are tested up to ery and avoid the spread of fluid droplets to other areas, a final concentration of 1:1,000 (wt/vol). Sensation (usually itching) pollen exposure simulating natural exposures has been con is usually the first to occur followed by erythema and edema ducted in large exposure chambers or rooms. Recording the duration of 281 Procedure itching may add more objectivity to this measurement. Nasal challenges should be conducted in a quiet room with Quantitative measures include tear volume, amount of mucus, temperature and humidity being recorded. The subject should palpebral and/or bulbar conjunctival hyperemia or erythema, be allowed to accommodate to the environment for at least 30 edema, or surface sensation of itching. This is followed by a control challenge millimeter reticule of the slit-lamp microscope. If the nasal airway resis ments are made of the lower lid and bulbar conjunctivae. Otherwise, testing continues with increasing con composition and cytology (ie, inflammatory cells, mediators, 282,283 centrations of the allergen challenge material and measure cytokines, specific IgE antibodies). Nasal challenges provide objective minutes for the next 10 to 15 minutes, every 5 minutes if evidence of clinical sensitivity when the diagnosis is in ques testing is continued beyond 15 minutes). Objective ancillary measures in evaluated by subjective symptoms and objective measure clude counting of sneezes and measurement of secretions. Specific (allergic) bronchial chal Over the years, many procedures for delivering allergen have lenge provides a measure of lower airway clinical sensitivity been used. The allergen can be applied as a dry or fluid when there is uncertainty or dispute. Guidelines for the performance of been placed or inhaled directly in the nasal mucosa but can be specific bronchial challenge include factors such as withhold difficult to distribute evenly and prevent inhalation into the ing certain medications before the test, determining the initial lower airways. In general, the initial comparison to a placebo-controlled challenge usually per concentration can be 10 to 100-fold more concentrated than formed the day before the specific challenge, and, optionally, the concentration that produced a 2 reaction with a wheal repetition of methacholine challenge 24 to 48 hours after greater than 5 mm (eg, an initial concentration of 0. Additionally, possible new asthma trig 309 may be useful for planning the duration of exposure. Before implementation of a specific Procedures bronchial challenge, many centers elect to determine the Because suspected allergens or agents in the home or work degree of nonspecific bronchial hyperresponsiveness as a place have different physical configurations, protocols for guide to allergen dosage and duration of allergen challenge. For soluble sured, dose increments of methacholine or histamine are allergens, aerosolization is the preferred technique. The precautions and A greater fall indicates bronchial lability that can affect test preparations recommended for specific new challenges are results, and further testing should be postponed until the identical to those for nonspecific testing (eg, methacholine, underlying asthma is stabilized. Pulmonary function tests are best performed 10 to of inhaled cromolyn and steroids is preferably discontinued 1 15 minutes after aerosol challenge. Antihistamines should considered a positive response, and the testing is stopped if be withheld for at least 72 hours. In 20 24 to 48 hours if the presence of a late response needs to be haled short-acting agonists should be given to restore 2 observed. Some clinicians repeat methacholine challenge 24 Specific bronchial challenge should be performed only in a to 48 hours after specific challenge for evaluation of induced medically supervised setting, usually a hospital or research bronchial hyperresponsiveness. Occupational challenge testing re absence from work, the worker returns to his/her job for a quires special precautions with respect to the innate toxicity period of 1 to 2 weeks. This is accomplished by visual inspection, but a Hygienists sets the threshold limit value and short-term ex 314 computer-based pattern recognition system having the advan posure limit for many occupational agents. If possible, the level of the suspected agent is Animal exposure challenges measured in the workplace, and this level is used to guide the Animal exposure challenges are used primarily in research dose for testing so that unrealistically high concentrations are settings to determine the efficacy of medication regimens or not inappropriately used. If the subject has a history of a severe, gens vary widely, the cat room is still considered a conve immediate reaction, exposure should be shorter and more nient and valid challenge technique that closely approximates incremental. These may define specific phenotypes or in some cases Asthma, which reviewed general principles for specific bron 318 predict severity. The nature of workplace exposure should be simulated specific inflammatory events. Special protocols and closed circuit tory markers is emerging as a common clinical paradigm.