Astralean
Isaac O. Karikari, MD
- Resident
- Division of Neurosurgery
- Duke University School of Medicine
- Durham, North Carolina
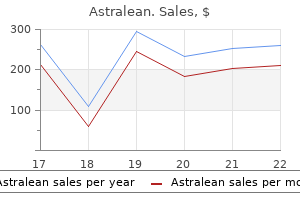
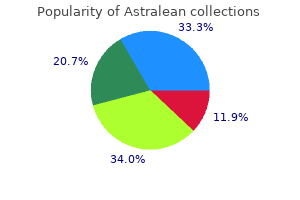
Non-invasive diagnosis of risk in dengue patients using bioelectrical impedance analysis and artificial neural network weight loss resources order discount astralean line. Modeling of hemoglobin in dengue fever and dengue hemorrhagic fever using bioelectrical impedance weight loss pills quick trim cheap astralean 40 mcg on line. Prevalence of dengue fever and dengue hemorrhagic fever in Hospital Tengku Ampuan Rahimah weight loss programs order 40 mcg astralean with mastercard, Klang weight loss pills that work over the counter generic 40 mcg astralean with visa, Selangor weight loss pills by prescription buy astralean cheap online, Malaysia weight loss pills seen on dr oz trusted 40 mcg astralean. Localization of dengue virus in naturally infected human tissues, by immunohistochemistry and in situ hybridization. Evaluation of a capture screening enzyme-linked immunosorbent assay for combined determination of immunoglobulin M and G antibodies produced during Dengue infection. Nonsubstrate based inhibitors of dengue virus serine protease: a molecular docking approach study binding interactions between protease and inhibitors. Asia Pacific Journal of Molecular Biology and Biotechnology 2007;15(2):53-9. Transovarial transmission of dengue virus in Aedes aegypti and Aedes albopictus in relation dengue outbreak in an urban area in Malaysia. Structure-based and ligand-based virtual screening of novel methyltransferase inhibitors of the dengue virus. Community vulnerability on dengue and its association with climate variability in Malaysia: a public health approach. Application of geographical information system for spatial-temporal mapping: a case study of dengue cases in Seremban, Negeri Sembilan, Malaysia. Chikungunya infection in Malaysia: comparison with dengue infection in adults and predictors of persistent arthralgia. The place of health and the health of place: dengue fever and urban governance in Putrajaya, Malaysia. Epidemiological and clinical features of dengue versus other acute febrile illnesses amongst patients seen at government polyclinics. Awareness of dengue and practice of dengue control among the semi-urban community: a cross sectional survey. A review of dengue fever incidence in Kota Bharu, Kelantan, Malaysia during the years 1998-2003. The role of an emergency department short-stay ward in the management of dengue fever: a case-control study in a university hospital. Co-infection of dengue virus and chikungunya virus in two patients with acute febrile illness. Measurement of dengue epidemic spreading pattern using density analysis method: retrospective spatial statistical study of dengue in Subang Jaya, Malaysia, 2006-2010. A case-control study on factors affecting the incidence of dengue fever in Johor Bahru. Audit of haemorrhagic manifestations in dengue infection and its correlation with bleeding profile. Serial tourniquet testing in dengue haemorrhagic fever-How clinically useful is it? Asian Oceanian Journal of Pediatrics and Child Health 2004;3(1):16-25. Field evaluation on the effectiveness of a modified approach of chemical fogging against the conventional fogging in controlling dengue outbreak. The role of virological surveillance of dengue serotypes for the prediction of dengue outbreak. Review of dengue hemorrhagic fever fatal cases seen among adults: a retrospective study. Antigenic cell associated dengue 2 virus proteins detected in vitro using dengue fever patients sera. Use of multiple data sources estimate the economic cost of dengue illness in Malaysia. Carica papaya leaves juice significantly accelerates the rate of increase in platelet count among patients with dengue fever and dengue haemorrhagic fever. Dengue infection in pregnancy: prevalence, vertical transmission, and pregnancy outcome. The clinical features and outcomes of acute liver failure associated with dengue infection in adults: a case series. Risk factors associated with development of dengue haemorrhagic fever or dengue shock syndrome in adults in Hospital Tengku Ampuan Afzan Kuantan. Differential expression of aldolase, alpha tubulin and thioredoxin peroxidase in peripheral blood mononuclear cells from dengue fever and dengue hemorrhagic fever patients. The use of two-dimension electrophoresis identify serum biomarkers from patients with dengue haemorrhagic fever. Predictive value of thrombocytopaenia in the diagnosis of dengue infection in outpatient settings. Prevalence of non-dengue thrombocytopaenia among adult patients presenting with acute febrile illness in primary outpatient clinics. Clinical features of acute febrile thrombocytopaenia among patients attending primary care clinics. Evolutionary history of Dengue virus type 4: insights into genotype phylodynamics. Molecular typing of dengue viruses circulating on the East Coast of Peninsular Malaysia from 2005 2009. Antibody neutralization and viral virulence in recurring dengue virus type 2 outbreaks. Behavioural factors influencing the dengue infection: the study among students in the higher learning institution. Sensitivity of Aedes albopictus C6/36 cells line for the detection and infectivity titration of dengue virus. International Proceedings of Economics Development & Research 2011;1:345-9. Atrial fibrillation as a complication of dengue hemorrhagic fever: non-self-limiting manifestation. A case of mixed infections in a patient presenting with acute febrile illness in the tropics. The mosquitoes are genetically engineered die at the larval stage in the absence of the antibiotic tetracycline, which acts as a chemical switch allow breeding in the laboratory. Claims about suppression of the wild mosquito population are largely based on unpublished results Oxitec has published no results from its experiments in Brazil in scientific journals, although it has been conducting these experiments since 2011 and has made frequent claims of success in press releases. Results from the Cayman Islands suggest this technology is very ineffective at reducing wild mosquito population numbers, requiring 2. In the Cayman Islands, the mosquito population was observed increase in the control area as the population in the release area decreased, and this is also seen in the very limited information available from Brazil. Oxitec originally hid this information43 but later admitted an 18% survival rate of larvae fed on cat food in a published paper. However, a number of studies have found that Aedes aegypti mosquitoes can breed in septic tanks where there can be high levels of contamination with antibiotics such as tetracycline. In the Cayman Islands, mechanical sorting led about 5,000 biting female mosquitoes in every million males (additional sorting was then performed by hand before release). If these bacteria become resistant tetracycline as a result, some human or animal diseases may become difficult treat. This issue has not been considered in risk assessments in either Panama or Brazil. Oxitec has not published any information about the origins of the Mexican strain and it does not appear have tested the back-crossed strain for insecticide-resistance or disease transmission properties. If the genetically modified strain is a more effective vector of disease than the established strain where it is introduced, this could pose a risk. Considerations in the Design of Clinical Trials Test Novel Entomological Approaches Dengue Control. Simulations compare efficacies of tetravalent dengue vaccines and mosquito vector control. High Level of Vector Competence of Aedes aegypti and Aedes albopictus from Ten American Countries as a Crucial Factor in the Spread of Chikungunya Virus. Ethical, legal and social issues of genetically modified disease vectors in public health. Efeito da qualidade da agua no ciclo de vida e na atracao para oviposicao de Aedes aegypti (L. Septic tanks as larval habitats for the mosquitoes Aedes aegypti and Culex quinquefasciatus in Playa-Playita, Puerto Rico. Mosquito larvae (Culicidae) and other Diptera associated with containers, storm drains, and sewage treatment plants in the Florida Keys, Monroe County, Florida. Unusual productivity of Aedes aegypti in septic tanks and its implications for dengue control. Conditional Control of Gene Expression in the Respiratory Epithelium: A Cautionary Note. Ghosh (2014) Insects represent a link between food animal farms and the urban environment for antibiotic resistance traits. This study investigated the factors affecting breeding habitats and the relationship with transovarial dengue virus in larvae of Aedes aegypti and Ae. Methods: Larval surveillance was conducted in dengue outbreak areas in Malaysia from 2008 until 2009. Sampling was carried out based on habitat type, water condition (substrate type), canopy coverage, temperature and pH at breeding habitats. Results: A total of 789 breeding habitats were identified during this study and the majority of these breeding sites were plastic containers (57. Interpretation & conclusion: this study indicated the presence of transovarial transmission of dengue virus in immature Ae. This study also showed that combination of water conditions, canopy coverage, temperature and pH of breeding habitats were the factors affecting the larval population. The study suggested that larval survey programme could serve as a tool not only monitor the local dengue vector distribution but also provide objective information for taking appropriate action by the community against dengue vectors. Since then dengue toes and destruction of their breeding places contain has remained endemic, with one or more of the four den an outbreak. Transovarial transmission of dengue virus Each pool of mosquito larvae was placed in a nu in the Aedes vectors is now a well-documented phenom clease-free 1. For positive control, an emphasise on the importance of larval control since the equal volume of cultured cells infected with dengue virus immature stages may become the reservoir of the virus was used and for negative control, uninfected cultured cells during the inter-epidemic periods. Container index was worked out as per standard volts and staining with ethidium bromide. Mosquito larvae collected in the sur viewed under ultraviolet illuminator (Ultra Lum Inc, Cali vey were identified using standard taxonomic keys5. Dengue type-specific primers used in this 70oC for future virus isolation studies. The mosquito study were commercially synthesized (D1S and D1C; D2S larvae pools were assayed for dengue virus detection by and D2C; D3S and D3C; D4S and D4C)7. Serotyping of the dengue positive pools were sults were analysed by 6 gel electrophoresis. These sites included man-made habitats such Rohani et al: Eco-virological survey of Aedes mosquito in Malaysia 329 Fig. Among these sites examined, plastic containers were the most preferred breeding sites (57. Significant correla for shaded and open canopy and slightly less for partially tion between substrate type condition and larvae popula shaded canopy, whereas in the case of Ae. The larval population was found highest in breed ing habitat which was partially shaded, followed by open habitat and the lowest was at fully shaded habitat. The results also clearly demonstrated that for all types of canopy, the larval population of Ae. The effect of temperature of the breeding sites in re lation larval population for both the species was also examined. Our findings showed that breeding activity was highest for both the species in breeding sites having wa ter temperature between 25 and 30?C (Fig. Only dengue 3 was detected in infected pools (5-pools) However, larval population for both the species was not of Ae. However, larval population for both the species was not significantly correlated (p >0. On the contrary, with dengue virus and of these positive pools, 18 were of the study on a nationwide Aedes larval survey carried out Rohani et al: Eco-virological survey of Aedes mosquito in Malaysia 331 in the years 1988?89 in peninsular Malaysia reported that albopictus might suggest that factors other than light is the house index and breteau index for both Ae. Our findings with respect canopy relation mosquito breeding sites) is now becoming an type are in general agreement with the finding of Lee15 important control/preventive measure in the battle against who reported that even partially closed containers had dengue. It is well-known that the primary dengue vector, larvae breeding in them and only complete coverage of Ae. Aedes mosquitoes breed in water collections ture could be one of the factors that determine suitability in artificial containers such as plastic cups, used tyres, of breeding habitats for both the species especially for broken bottles, flower pots, etc. Lee and pable of breeding profusely in natural breeding sites hav Rohani4 showed that transovarial dengue virus in wild ing a wide range of water condition (substrate type) from larvae was associated with dengue outbreak. Aedes aegypti larvae were is, therefore, necessary in order understand if such phe also detected in almost all the breeding sites, demonstrat nomenon could have a role play in facilitating the vi ing that container-breeding Aedes have the ability breed rus persist during inter-epidemic periods. Aedes aegypti population the study also clearly indicated that dengue-infected however was very much lower compared Ae. It is well-recog affected by the substrate type, and therefore, less selec nized that community participation is the key success tive with regards their breeding site as compared Ae. This finding was almost similar study done by the dengue vector surveillance programme serves as a Chen et al10 and Lee9 in Malaysia which reported that tool not only monitor the local dengue vector distribu Aedes larvae preferred breed in clear, but not necessar tion but also provide objective information for taking ily clean water. The lower in number of Malaysia for permission publish this paper and the Di larval population compared larval population of Ae.
Many of the estimates have a high degree of uncertainty and will likely change as more high quality data become available weight loss pills uk 2015 best order for astralean. However weight loss 7-day juice cleanse astralean 40 mcg otc, they provide reasonable estimates of the clinical benefits and harms relative weight loss pills qsymia order astralean discount each other weight loss pills yellow jackets purchase genuine astralean line. Thus weight loss 08844 order astralean amex, we know with a high degree of certainty that all forms of supplemental screening find additional breast cancers weight loss pills ketone purchase 40 mcg astralean mastercard. Most of the cancers are small, lymph node negative, and thus are potentially curable. The major unanswered question is whether the identification of additional cancers through supplemental screening improves outcomes for women. Some advocates of supplemental screening will argue that the majority of the cancers identified through supplemental screening are early stage cancers with an excellent prognosis following treatment. These represent the spectrum of cancers identified with mammography that led the reduction in mortality seen with the randomized trials of screening mammography. In their view, there can be no question that patient outcomes will be improved with supplemental screening. Others will argue that many of these supplemental screen-detected cancers would have been cured when detected on physical exam or subsequent screening mammograms and that some of these cancers represent overdiagnosis, which leads net harm for the patient. They will highlight the growing evidence for significant overdiagnosis with mammography alone. The search timeframe spanned from April 11, 2013 October 18, 2013, with 150 records identified. The majority of these initial results (n=108) were excluded due inappropriate patient populations. Following removal of duplicate citations and initial evaluation, full-text review was performed on six retrieved articles. A single study was found be relevant the scope of this review, and is discussed in detail below. We developed a cohort model address this gap, focusing on the clinical and economic outcomes of supplemental screening in women with dense breast tissue and a negative mammogram. Information on the economic impact of any screening strategy for women with dense breast tissue is also quite limited. We nevertheless summarize the published evidence relevant the scope of this review in the section below. Tosteson and colleagues used modeling evaluate the cost-effectiveness of different screening strategies using digital mammography vs. In addition, 72% of women in the study sample were age <50, which is not reflective of the age distribution of women in the general screening population or of the subset with dense breast tissue. Costs were estimated for screening and biopsy based on billed charges insurers, and totaled approximately $3. Neither study compared screening costs after passage of the law costs incurred before the law was passed. We therefore developed a cohort model perform a population-based, one-year analysis of clinical and economic outcomes specific New England. In the model we included all women age 40-74 except for those with certain risk factors (see Target Population below). We first conducted baseline analyses comparing the screening performance and costs for both digital and film mammography for all women undergoing screening. Then, we used the model compare the performance and costs of supplemental screening with each of the modalities of interest. For these analyses of supplemental screening, digital mammography was assumed for initial screening, as evidence indicates it is the current screening standard. We defined the supplemental screening population as a hypothetical cohort that was stratified into different levels of underlying breast cancer risk. Several more sophisticated risk assessment algorithms are available, but for modeling purposes we opted use a simplified risk algorithm based on just these three factors maximize the feasibility and potential generalizability of this approach (see Overall Breast Cancer Risk below). We had make several broad assumptions in designing the model that are important because they limit the ability of the model capture the nuances of patient behavior and the many variations in clinical care patterns that occur for individual patients. For example, we assumed perfect compliance for both mammography and supplemental screening in this analysis. While it is the case that actual compliance is always less than 100%, differences across studies in the definition of the time interval within which women are considered compliant as well as considerations of what 183 constitutes screening vs. The model assumes that supplemental screening would occur immediately after a negative mammography result, and that one year of follow-up is available as the reference standard for both mammography and supplemental screening results. For mammography, we needed estimate as inputs several important numbers based on our review of the clinical evidence, including the number of cancers detected. We developed similar inputs for each supplemental screening strategy, but we made a simplifying assumption that all positive supplemental screening tests would result in immediate biopsy, and so did not estimate recall rates (which would equal biopsy rates in this case) or false-positive results without biopsy. As noted in this review, supplemental screening has the potential detect both cancers missed by mammography and additional cancers that would not have presented during the interval between mammography Institute for Clinical & Economic Review, 2013 Page 81 screenings; we therefore included both types of cancer in our estimates for each supplemental modality. Target Population the population we modeled included all women age 40-74 except for those with known genetic susceptibility, a personal history of breast cancer, and/or a history of mantle radiation the chest. On a population basis, approximately 46% of the New England screening population would have heterogeneously dense (1. Table 17: Estimates of overall screening population and target population for supplemental screening, by age. The percentage of women with dense breast tissue and a close family history was estimated be 22. Based on the risk categories described above, we estimate that, of all New England women with dense breast tissue and a negative digital mammogram, 33% would be low-risk, 54% moderate-risk and 13% high-risk. These proportions are displayed in Figure 2 on the following page along with the relevant estimated population sizes for each risk group. The rate of interval cancers in most screening populations is approximately 1 per 1,000 women 112,192 screened. Cancer detection rates were divided by cancer yield estimates obtain an estimate of the total number of biopsies performed for each modality. Because the performance of screening tests has been found improve with increasing disease 193 prevalence, we also assumed that all of these measures. We developed estimates for each risk subgroup that would equate the overall levels described above when weighted by population size. We estimated that between 10-30% of biopsy-detected cancers would be cases of overdiagnosis, based on the 91,95,194,195 range generally reported in the literature. We present the lower and upper boundaries of this range for each screening scenario evaluated. Test/Procedure Components Payment Source(s) Screening Bilateral exam, Medicare fee schedule Mammography computer-aided Film detection $91. For each supplemental screening strategy, costs of interest included those of screening, biopsy, and diagnosis of interval cancers. To facilitate comparisons, we present all clinical findings on a per 1,000 women screened basis, and costs are presented as an average per woman screened. As shown in the table, digital mammography results in a small increase in the number of cancers detected (3. Rates of false-positive results with or without biopsy were somewhat higher for digital mammography, owing its slightly lower specificity overall. Taking into account differences between digital and film mammography, approximately 12 biopsies would need be performed with digital mammography in order detect one additional cancer over film mammography. For example, cancer occurred at a rate of approximately 5 per 1000 in women with extremely dense breasts, vs. The increase in cancers detected, while still small, was threefold that observed in the overall cohort. Among women with dense breast tissue, the number of biopsies required with digital mammography detect each additional cancer as compared film mammography was much lower than that for the overall population (5 vs. As discussed previously, neither recalls nor false-positives without biopsy were estimated for these analyses, as all positive supplemental screening results were assumed result in biopsy. Costs were assumed differ, however, and are presented separately at the bottom of the table. Each of the supplemental modalities would identify nearly all of the cancers missed by mammography. Table 22: Clinical outcomes and costs of supplemental screening in New England in all women with dense breast tissue and negative mammography: vs. As in the overall population, each of the supplemental strategies would detect nearly all of the cancers missed by mammography. Table 23: Clinical outcomes and costs of supplemental screening in New England in women at low overall breast cancer risk with dense breast tissue and negative mammography: vs. The higher prevalence of cancer in this subgroup is associated with higher rates of biopsy and false-positive results for all tests. There was some separation in the number of interval cancers that would have been missed by supplemental screening (0. Table 24: Clinical outcomes and costs of supplemental screening in New England in women at moderate overall breast cancer risk with dense breast tissue and negative mammography: vs. Table 25: Clinical outcomes and costs of supplemental screening in New England in women at high overall breast cancer risk with dense breast tissue and negative mammography: vs. Differences in false-positive rates are also magnified in the high-risk population. While differences between modalities in the number of additional cancers detected remain relatively stable with increasing risk, differences in rates of false-positive biopsy become more pronounced. Figure 3: Selected incremental effects of supplemental screening, by screening modality and overall breast cancer risk. Table 26: Population-based estimates of incremental clinical impact of supplemental screening among New England women with dense breast tissue and negative mammography results, by supplemental screening modality and overall breast cancer risk. For example, the numbers of total and false-positive biopsies would be similar in these two subgroups, but supplemental screening would detect 350 400 more cancers in the high-risk population despite the fact that it is 40% the size of the low-risk group. The estimated budgetary impact New England of supplemental screening in all women with dense breasts and negative mammography can be found in Figure 4 on the following page. The annual cost of digital mammography screening, including costs of mammography, diagnostic workup, and biopsy, is estimated total approximately $576 million. Figure 4: Costs of digital mammography and supplemental screening among New England women, by screening modality. Figure 5 on the following page shows the additional costs of supplemental screening when limited women in the high risk category. If supplemental screening were limited women age 50-74 with dense breast tissue, a family history in a first degree relative, and a negative digital mammogram. However, the potential yield of additional cancers detected in this subgroup would be comparable or better than with digital mammography alone. Increases in cost would be lower with the other supplemental modalities (5 Institute for Clinical & Economic Review, 2013 Page 96 7%), but the additional cancer yield would also be lower (1,000 1,100 additional cancers detected over digital mammography alone). Findings such as these are important consider in any evaluation of the tradeoffs of supplemental screening, including numbers of biopsies required, additional cancers detected and missed, and screening costs. Figure 5: Costs of digital mammography and supplemental screening among high-risk New England women only, by screening modality. First, as required by any modeling approach, we made a number of simplifying assumptions that may not truly reflect the use of either mammography or supplemental screening in clinical practice. These included screening behaviors and clinical decisions such as perfect compliance with both types of screening as well as referral for and performance of biopsy in 100% of women with positive supplemental screening results. These assumptions likely resulted in overestimates of rates of cancer detection and cost for both mammography and supplemental screening. However, these modalities have by and large not been studied exclusively in women with dense breast tissue and negative mammography who are at varying levels of overall breast cancer risk. This type of information will only be available through the conduct of longer-term randomized controlled trials or cohort studies comparing the benefits of supplemental screening digital mammography alone. For women with dense breast tissue, is the evidence adequate demonstrate that digital mammography offers superior diagnostic performance compared with film mammography? For women with dense breast tissue, is the evidence adequate demonstrate that, compared with film mammography, digital mammography substantially reduces the risk of masking of breast cancers? For women with dense breast tissue with an overall low risk of breast cancer who have a negative screening digital mammogram, is the evidence adequate demonstrate that supplemental screening with any technology provides more benefit than harm compared with no supplemental screening? For women with dense breast tissue with an overall moderate risk of breast cancer who have a negative screening digital mammogram, is the evidence adequate demonstrate that supplemental screening with any technology provides more benefit than harm compared with no supplemental screening? As the underlying risk of cancer increases, Council members were more likely believe that the net health benefits of supplemental screening were positive for most women. Council members who voted yes, however, stressed that the overall poor quality of evidence on patient outcomes made it difficult determine precisely at what risk threshold supplemental screening would be expected have a positive net benefit. For women with dense breast tissue with an overall high risk of breast cancer who have a negative screening digital mammogram, is the evidence adequate demonstrate that supplemental screening with any technology provides more benefit than harm compared with no supplemental screening? Considering both the strength of evidence and the magnitude of potential comparative clinical benefits and harms of these four imaging modalities, if supplemental screening were be performed for women with dense breast tissue who are at high risk of breast cancer, please rank in order, from highest lowest preference, the tests you would recommend a patient and her clinician. Health benefits and harms considered should include additional cancers detected and the possible impact on patient outcomes; false negative test results that miss critically significant cancers; false positive test results with their impact of unnecessary biopsies and anxiety; and overdiagnosis. The comparative net health benefit requires consideration of all relevant potential benefits and harms as described in the report. Consideration of the economic impact of supplemental screening should be broadened consider the societal perspective, including considerations for missed work, transportation, and other costs. Some states in New England lack the capacity sustain increased demand for public health screening, particularly in northern parts of the region. The main themes and recommended best practices from the conversation are summarized in the sections below. Experts on the Roundtable noted that it is important for clinicians and women understand that dense breast tissue conveys some increased risk for breast cancer but by itself is not a reason Institute for Clinical & Economic Review, 2013 Page 103 consider a woman at high risk of developing the disease. Roundtable experts from Connecticut, the only state in New England enact a breast density notification law and mandate coverage for screening ultrasound in women with dense breasts, noted that practices vary in how they handle referrals for supplemental screening.
The helping health consumers reduce their fnancial People living with metastatic breast cancer understanding Centrelink entitlements for which burden weight loss pills gnc discount astralean 40 mcg online. The incurable nature of metastatic long hold times on the telephone or difculty treatment and care when compared weight loss pills ziszonade order astralean paypal women breast cancer means that additional fnancial visiting a Centrelink ofce when unwell weight loss breastfeeding purchase cheap astralean line. Long Women living in a rural or regional area face without private health insurance approximately burdens include the ongoing costs of treatment weight loss 7 months discount astralean 40 mcg overnight delivery, waiting times for payments weight loss jars buy cheap astralean line start is also a issues such as travelling long distances weight loss 4 pills reviews purchase astralean 40 mcg visa, staying $7,000 for insured women compared with difculty planning for the future, not knowing reported issue. Women phone and in physical locations) would assist with the costs for some women amounting Some women fnd that paying for cancer living with metastatic breast cancer will share people with cancer and other chronic illnesses more than $21,000. Women with private health treatment and its associated costs pushes many fnancial pressures in common with by being able provide them with tailored insurance paid approximately 10 times as much them the brink. This as women without private health insurance for on government benefts, charity handouts these pressures are amplifed by the nature of would streamline the process for people living their direct medical costs at $3,723 compared and emergency help from family, friends and metastatic breast cancer and add the burden. Even an expense as Accessing government assistance through them get the help which they are entitled. Women have Cancer Council Victoria found that costs of reported inconsistencies, lengthy wait times, 30 31 References 1 Australian Bureau of Statistics, 2016. For private health insurance companies 2 burden people with metastatic disease Cancer Council Victoria, 2016. Private health insurance companies better drugs are reviewed ensure that (2016). Characteristics of Employment, Australians can access medications in a Australia, August 2016. Documenting patterns of breast reconstruction by private health insurance companies For health service providers in Australia: the national picture. Documenting patterns of breast reconstruction of payment should be in addition the having treatment in the private health in Australia: the national picture. Documenting patterns of breast reconstruction of any proposed procedures prior in Australia: the national picture. Characteristics of Employment, refect the cost of providing services Australia, August 2016. This advice should cost of travelling away from home for the-government-should-do-about-it/ 15 August 2017. Special thanks are owed the 15 women who agreed share their personal stories as case studies for the report: Christie, Dannette, Farrah, Georgie, Helen, Jill, Karen, Kylie, Lisa, Louise, Lynne, Marie, Penny, Ruth and Susan. Thank you the photographers who generously provided their time and skills photograph the women featured in the case studies. Photography by Andrew Burn, Diane Kitanoski (Love Kit Photography), Melissa Drummond, Paul Dunlop, Sylvia Liber, Victoria Fitzmaurice (Essence Images) and Breast Cancer Network Australia. We encourage you review the recommendations outlined in this report and consider how you can help reduce the fnancial impact of breast cancer. We would welcome your commitment and contribution and look forward working with you help ensure a better journey for all Australians afected by breast cancer. Who contact For media enquiries: Penelope Davies Media Manager Phone: (03) 9805 2576 Email: pdavies@bcna. Improved imaging and increased screening uptake have led detect smaller cancers. Publication costs for this article were supported by the ecancer Global Foundation. This is an Open Access ment of patient outcome, of better communication skills and quality of life for women. This award was given by Paolo Veronesi, after a moving reproduction in any medium, provided the original introduction which culminated with the following words of Professor Umberto Veronesi: work is properly cited. My duty, the duty of all doctors, is listen and be part of the emotions of those we treat every day. Martine Piccart-Gebhart (Institut Jules Bordet, Belgium) presented news about systemic therapies. Christos Sotiriou (Institut Jules Bordet, Belgium) focussed on the genomic risk stratification of early relapse. Intratumour heterogeneity (genetic distance, lethal sub-clones in the primary tumour and genome instability) and genome evolution are going give us information about the risk of relapse. Interestingly, there also appears be a possible application for artificial intelligence and machine learning in this field of prediction [39]. Research priorities are the identification and the evaluation of biomarkers that could allow the best treatment for the patient [50?54]. Moreover, it is necessary encourage effective communi cation between patients and their physicians about the pros and cons of treatment versus surveillance. Emerging molecular tools offer the potential tailor treatment according biology. It is very important carefully select the study design, statistical techniques and also be aware of the limitations of trial data. Currently, emerging clinical biomarkers may predict the response these drugs. Combinations of immunotherapy with chemotherapy have been investigated in the advanced setting. It should be considered that surrogate endpoints do not consistently correlate with long term endpoints [59]. Some studies demonstrated major sensitivity carboplatin [61] but in others, it is less evident (GeparSixto). Bahadir Gulluoglu (Marmara University School of Medicine, Turkey) focussed his presentation on the impact of older age on local treat ment decisions. Radiotherapy for early breast cancer Timothy J Whelan (McMaster University, Canada) remarked that breast irradiation in some patients may be omitted. There are also trials evaluating the elimination of regional nodal radiotherapy in patients with limited node-positive disease and low biological risk. John H Maduro (University Medical Centre Groningen, the Netherlands) spoke about the potential role of proton irradiation compared conventional photon irradiation. Protons are charged particles able deliver the dose a specified depth where they stop, with a reduction of cardiac and pulmonary toxicity [82]. Nowadays, however, even if there has been a clear increase in proton facilities in recent years, the availability remains scarce and the costs high. There is emerging evidence that metabolomic profiling may have the ability further stratify risk within existing genomic assay determined risk categories [88, 89]. Benefits appeared similar across different bisphosphonates tested suggesting a class effect. These favourable outcomes increase the importance of risk stratification minimise over and under treatment, and de-escalation strategies potentially further reduce the toxicities of therapy. However, it is necessary consider the short-term toxicities, as well as the long-term ones, which determine a worsening of quality of life [98]. In these terms, the correct management of therapy and also integrative therapies which can help reduce the impact of the side effects assume great importance [99]. Non-medical factors, like underemployment, socioeconomic status and financial toxicity can also negatively impact on health outcome and quality of life [100]. Therapies should be effective, offer value, result in meaningful outcomes and be available. Choi J, Laws A, and Hu J, et al (2019) Margins in breast-conserving surgery after neoadjuvant therapy Ann Surg Oncol 25(12) 3541 3547 doi. Cuzick J, Dowsett M, and Pineda S, et al (2016) Prognostic value of a combined estrogen receptor, progesterone receptor, Ki-67, and human epidermal growth factor receptor 2 immunohistochemical score and comparison with the Genomic Health recurrence score in early breast cancer J Clin Oncol 29(32) 4273?4278 doi. Loi S, Drubay D, and Adams S, et al (2019) Tumor-infiltrating lymphocytes and prognosis: a pooled individual patient analysis of early stage triple-negative breast cancers J Clin Oncol 37(7) 559?569 doi. Denkert C (2018) Tumour-infiltrating lymphocytes and prognosis in different subtypes of breast cancer: a pooled analysis of 3771 patients treated with neoadjuvant therapy Lancet Oncol 19(1) 40?50 doi. Zou J, Huss M, and Abid A, et al (2018) A primer on deep learning in genomics Nat Genet 51(1) 12?18 doi. Denkert C, von Minckwitz G, and Darb-Esfahani S, et al (2018) Tumour-infiltrating lymphocytes and prognosis in different subtypes of breast cancer: a pooled analysis of 3771 patients treated with neoadjuvant therapy Lancet Oncol 19(1) 40?50 doi. Matuschek C, Bolke E, and Haussmann J, et al (2017) the benefit of adjuvant radiotherapy after breast conserving surgery in older patients with low risk breast cancer a meta-analysis of randomized trials Radiat Oncol 12(1) 60 doi. Wickberg A, Liljegren G, and Killander F, et al (2018) Omitting radiotherapy in women? Choi J, Laws A, and Hu J, et al (2018) Margins in breast-conserving surgery after neoadjuvant therapy Ann Surg Oncol 25(12) 3541 3547 doi. Feliciano Y, Mamtani A, and Morrow M, et al (2017) Do calcifications seen on mammography after neoadjuvant chemotherapy for breast cancer always need be excised? Omarini C, Guaitoli G, and Noventa S, et al (2017) Impact of time surgery after neoadjuvant chemotherapy in operable breast cancer patients Eur J Surg Oncol 43(4) 613?618 doi. Rack B (2014) Circulating tumor cells predict survival in early average-to-high risk breast cancer patients J Natl Cancer Inst 106(9) [doi/10. Oakman C (2011) Identification of a serum-detectable metabolomic fingerprint potentially correlated with the presence of micro metastatic disease in early breast cancer patients at varying risks of disease relapse by traditional prognostic methods Ann Oncol 22(6) 1295?1301 doi. Tenori L (2015) Serum metabolomic profiles evaluated after surgery may identify patients with oestrogen receptor negative early breast cancer at increased risk of disease recurrence. For Injection: 150 mg lyophilized powder in a single-dose vial for function prior and during treatment. The incidence and severity was highest in patients receiving Herceptin with anthracycline-containing chemotherapy regimens. Evaluate left ventricular function in all patients prior and during treatment with Herceptin. Discontinue Herceptin treatment in patients receiving adjuvant therapy and withhold Herceptin in patients with metastatic disease for clinically significant decrease in left ventricular function [see Dosage and Administration (2. Infusion Reactions; Pulmonary Toxicity Herceptin administration can result in serious and fatal infusion reactions and pulmonary toxicity. Discontinue Herceptin for anaphylaxis, angioedema, interstitial pneumonitis, or acute respiratory distress syndrome [see Warnings and Precautions (5. Embryo-Fetal Toxicity Exposure Herceptin during pregnancy can result in oligohydramnios and oligohydramnios sequence manifesting as pulmonary hypoplasia, skeletal abnormalities, and neonatal death. Advise patients of these risks and the need for effective contraception [see Warnings and Precautions (5. Improper assay performance, including use of suboptimally fixed tissue, failure utilize specified reagents, deviation from specific assay instructions, and failure include appropriate controls for assay validation, can lead unreliable results. Adjuvant Treatment, Breast Cancer Administer according one of the following doses and schedules for a total of 52 weeks of Herceptin therapy: During and following paclitaxel, docetaxel, or docetaxel/carboplatin. Initial dose of 4 mg/kg as an intravenous infusion over 90 minutes then at 2 mg/kg as an intravenous infusion over 30 minutes weekly during chemotherapy for the first 12 weeks (paclitaxel or docetaxel) or 18 weeks (docetaxel/carboplatin). As a single agent within three weeks following completion of multi-modality, anthracycline-based chemotherapy regimens. Administer Herceptin, alone or in combination with paclitaxel, at an initial dose of 4 mg/kg as a 90-minute intravenous infusion followed by subsequent once weekly doses of 2 mg/kg as 30-minute intravenous infusions until disease progression. Administer Herceptin at an initial dose of 8 mg/kg as a 90-minute intravenous infusion followed by subsequent doses of 6 mg/kg as an intravenous infusion over 30?90 minutes every three weeks until disease progression [see Dosage and Administration (2. Subsequent Herceptin maintenance doses should be administered 7 days or 21 days later according the weekly or three-weekly schedules, respectively. If the patient has missed a dose of Herceptin by more than one week, a re-loading dose of Herceptin should be administered over approximately 90 minutes (weekly schedule: 4 mg/kg; three weekly schedule: 8 mg/kg) as soon as possible. Subsequent Herceptin maintenance doses (weekly schedule: 2 mg/kg; three-weekly schedule 6 mg/kg) should be administered 7 days or 21 days later according the weekly or three-weekly schedules, respectively. Using a sterile syringe, slowly inject the 20 mL of diluent into the vial containing the lyophilized powder of Herceptin, which has a cake-like appearance. The reconstituted vial yields a solution for multiple-dose use, containing 21 mg/mL trastuzumab. The solution should be free of visible particulates, clear slightly opalescent and colorless pale yellow. Calculate the volume of the 21 mg/mL reconstituted Herceptin solution needed, withdraw this amount from the vial and add it an infusion bag containing 250 mL of 0. Use appropriate aseptic technique when performing the following reconstitution steps. The reconstituted vial yields a solution for single-dose use, containing 21 mg/mL trastuzumab. If not used immediately, store the 0 0 0 0 reconstituted Herceptin solution for up 24 hours at 2 C 8 C (36 F 46 F); discard any unused Herceptin after 24 hours. The highest absolute incidence occurs when Herceptin is administered with an anthracycline. The safety of continuation or resumption of Herceptin in patients with Herceptin-induced left ventricular cardiac dysfunction has not been studied. Patients who receive anthracycline after stopping Herceptin may also be at increased risk of cardiac dysfunction [see Drug Interactions (7) and Clinical Pharmacology (12. In Study 3 (one-year Herceptin treatment), the number of patients who discontinued Herceptin due cardiac toxicity at 12. Among 64 patients receiving adjuvant chemotherapy (Studies 1 and 2) who developed congestive heart failure, one patient died of cardiomyopathy, one patient died suddenly without documented etiology, and 33 patients were receiving cardiac medication at last follow-up. In post-marketing reports, serious and fatal infusion reactions have been reported. Severe reactions, which include bronchospasm, anaphylaxis, angioedema, hypoxia, and severe hypotension, were usually reported during or immediately following the initial infusion. However, the onset and clinical course were variable, including progressive worsening, initial improvement followed by 7 clinical deterioration, or delayed post-infusion events with rapid clinical deterioration.
This is primarily due weight loss using phentermine buy astralean 40 mcg on line the high costs of running vertical programs that would function at the previous level (100% of households inspected every three months) weight loss 08080 cheap astralean online, increased urbanization with peri-urban areas lacking in basic infrastructure weight loss pills ziszonade 40 mcg astralean fast delivery, the widespread use of nonbiodegradable items with a concurrent lack of adequate trash disposal and sanitary landfill systems weight loss pills jillian astralean 40 mcg low price, and governments struggling weight loss pills stars use purchase 40 mcg astralean amex control unplanned growth weight loss vs fat loss generic 40 mcg astralean amex. The primary activity of dengue control programs is the control of larval habitats of Ae. This approach relies heavily on community participation in control activities, yet most dengue control programs are unprepared develop and manage sustained community participation strategies. This report includes 11 examples of practices currently in use in several countries, nine from the Americas, one from Southeast Asia, and one of global application. The practices, written by individuals involved in the development and implementation of the practice, cover a wide range of activities that would be expected from an integrated dengue prevention and control program. These examples have been termed best practices since they have been evaluated for effectiveness and are in use as part of broader programs. These best practices are not intended be prescriptive nor can they, with the exception of the case definitions, clinical case management, and laboratory practices, be transferred from one setting another without prior field testing. The practices should also not be viewed as a panacea for dengue prevention and control. Rather, they are examples of specific components of several programs, developed in many cases according cultural and ecological circumstances. It is hoped that the inclusion of descriptions of the processes develop the practice in four of the 11 practices (Brazil, Vietnam, Mexico, and Dominican Republic) will provide sufficient information encourage other countries conduct similar operational research activities. The annexes in this document provide information on international organizations involved in dengue prevention and control, contact information for further information and technical assistance, and resources that can be found on the Internet. It is hoped that this document will stimulate further discussions on how strengthen dengue prevention and control actions that are implemented regularly rather than on an emergency basis, how sustain resources over several years so that truly effective control strategies can be tested and implemented, and how encourage routine monitoring and field evaluation of all activities so that program staff and affected communities know that the actions are effective at the individual or community level. In the region of the Americas the pattern follows what was seen in Asia 30 years ago. Today, dengue is the most important mosquito-borne viral disease affecting humans, with Aedes aegypti, the mosquito vector for the dengue viruses, found in nearly 100 tropical countries. Hyperendemicity, the presence of multiple circulating serotypes, is seen in most countries in the region, and epidemics caused by multiple serotypes are more frequent. Effective mosquito control is virtually nonexistent in most dengue-endemic countries, and emphasis has been placed on ultra-low volume insecticide space sprays for adult mosquito control, a relatively ineffective approach for controlling Ae. Major global demographic changes, primarily uncontrolled urbanization and concurrent population growth, have occurred, resulting in substandard housing and inadequate water, sewer, and waste management systems. There have been significant increases in the use of nonbiodegradable packaging, compounded by nonexistent or ineffective trash collection services. Increased travel by airplane has resulted in a constant exchange of dengue viruses and other pathogens. The reality of limited financial and human resources has resulted in a "crisis mentality" with emphasis on implementing emergency control methods in response epidemics rather than on developing programs prevent epidemic transmission. Because most national programs are not equipped manage the prevention and control aspects of a dengue program, heavy reliance continues be placed on chemical control methods and outdated strategies. The sad reality is that the majority of national dengue control programs are based on emergency responses epidemics, and there are no staff or resources implement integrated strategies for dengue prevention and control during interepidemic years. The vertical structure of most dengue programs, based upon vector control field workers visiting every household in a specific area on an established cycle (ideally four times a year), was developed 60 years ago for yellow fever eradication. Today, this structure is not possible given increasing urbanization, budgetary constraints, lack of personnel, the presence of increasing numbers of closed households (no one home during the day allow access the house or the premise), and householder rejection of the use of larvicides in domestic water-holding containers used store drinking water. This impact varies and can include loss of life; medical expenditures for hospitalization of patients; loss in productivity of the affected workforce; strain on health care services due sudden, high demand during an epidemic; considerable expenditures for large-scale emergency control actions; and loss of tourism as a result of negative publicity (Meltzer et al. Rather, these examples provide a snapshot of efforts currently underway that have demonstrated some degree of effectiveness and sustainability. Infection with one of these serotypes provides lifelong immunity against that serotype, but it does not provide cross-protective immunity against the other three. A major challenge for disease surveillance and case diagnosis is that the dengue viruses produce asymptomatic infections and a spectrum of clinical illness ranging from a mild, nonspecific viral syndrome fatal hemorrhagic disease. It may present as an undifferentiated febrile illness with a 6 maculopapular rash (often seen in children), a mild febrile syndrome similar the flu, or the classical disease with two or more of the following manifestations: fever, headache, bone or joint pain, muscular pain, rash, pain behind the eyes, hemorrhagic manifestations. During dengue epidemics, hemorrhagic complications may also appear, such as bleeding from the gums, nosebleeds, and bruising. All three manifestations of circulatory failure must be present: rapid and weak pulse, narrow pulse pressure or hypotension for age of patient, and cold, clammy skin and altered mental state. R4) established a model for the prevention and control of dengue, with a goal of showing member states how move from vertical vector control models horizontal vector control programs. This is especially important given health sector reform efforts currently underway in the region, and the fact that most local health services, now responsible both politically and administratively for prevention programs, are not sufficiently established take on these programs. Local health departments, be it at the regional, state, or municipal levels, have generally not had access the levels of technical staff found at the central Ministry of Health offices, yet they are tasked with implementing the regional integrated strategy defined in 1994, and expanded upon in 1997, 1999, and 2001. R4) passed in September 2001, and delineates the 10 key elements (the Decalogue) of the regional integrated strategy. The global strategy delineates the five essential components of the global strategy. Organization of this Document In the following section, the conceptual framework for a comprehensive, integrated dengue prevention and control program is presented. These examples are intended illustrate not only what a best practice for the specific element is but, where possible, the process used develop the practice. Each best practice is an independent example, allowing the reader read individual practices without reading the entire section. The best practices are not intended be prescriptive approaches that will work in every setting. The latter set of best practices reflects local conditions that required new approaches effective dengue prevention and control, and therefore formative research. It is important keep in mind that the best practices presented in this document are examples of specific components of several programs and that no one dengue program was identified as being a model program. The series of best practices demonstrate that achieving an integrated dengue prevention and control program takes time, commitment, political will, and consistent efforts in working toward this goal. The conclusion, found in Section 4, presents some ideas for next steps, and additional resources can be found in the annexes. Conceptual Framework the conceptual framework for this document is a comprehensive, integrated dengue fever prevention and control that places equal weight, including fiscal and human resources, on all elements of the program. Comprehensive program strategies address several public health problems as part of the dengue control program; for example, combining Culex species control, a far greater nuisance mosquito, with Aedes control will provide benefits the dengue program since nuisance mosquito populations should be reduced. An integrated program uses all potential vector control techniques in the most effective, economical, and safe manner maintain vector populations at acceptable levels. Currently, most if not all countries in the Americas have a national plan of action for dengue prevention and control that, on paper, demonstrates some level of commitment an integrated strategy. However, operationally most programs function as vertical Aedes aegypti control programs implementing emergency mosquito control activities in response increasing cases of dengue. Larval habitats are increasing at an alarming rate for several reasons: the rapidly increasing costs of running vertical programs that function at previous levels, the widespread use of nonbiodegradable items with a concurrent lack of adequate trash disposal and sanitary landfill systems, increased urbanization with peri-urban areas lacking in basic infrastructure, and governments struggling control unplanned growth. These methods rely heavily on community participation in routine source reduction (the control of mosquito habitats) activities, yet most dengue control programs are ill equipped develop and manage sustained community participation strategies. This commitment would include multiyear funding allow the program establish new policies and procedures, annual funding support formative and operations research, annual funding support community-based activities, and a programmatic emphasis on regular field evaluation of all program activities. Until this occurs, it is unlikely that there will be any change in current dengue transmission patterns since little programmatic support exists for the implementation of comprehensive, integrated dengue prevention and control using methods with demonstrated field efficacy. Advocacy and implementation of intersectoral actions between health, environment, and education as well as other sectors such as industry and commerce, tourism, legislation, and judiciary. Environmental management and addressing basic services such as water supply, disposal of used water, solid waste management, and disposal of used tires. Formal health training of professionals and workers both in the medical and social sciences. Emergency preparedness, establishing mechanisms, and plans face outbreaks and epidemics. Dengue program managers are dependent upon reporting mechanisms unique each department, and therefore the data collected may not overlap sufficiently. Epidemiological reports are sent, frequently by mail, the vector control department with a resulting one three-week lag in receipt (data collected during external evaluations of national dengue control programs, L. Passive surveillance is not sensitive enough for early detection of epidemics since not all clinical cases are correctly diagnosed, especially at the beginning of an outbreak when physicians may not suspect dengue, and mild cases may not enter the health care system at all. By the time a significant rise in the number of reported cases is detected, the epidemic may already be peaking or on the decline. These guidelines recommend that disease surveillance be an active system that uses both laboratory and clinical dengue surveillance activities provide early and precise information health officials. An active surveillance system 13 includes sentinel clinics, monitoring of cases of fever of undiagnosed origin, confirmation of cases by laboratory tests, and ongoing analysis of trends of reported cases. For those individuals with technical training in one field or the other (either epidemiology or vector control), triangulation of the data can be challenging. In reality, actions are often taken in isolation, with vector control staff using data obtained through entomological surveillance and the health services sector responding the clinical surveillance data. This results in delayed response emerging epidemic trends, inappropriate use of control methods. Although countries may have an intersectoral taskforce or commission, often these groups do not meet unless there is a dengue epidemic. Individual countries will need analyze current epidemiological and entomological reporting mechanisms and identify ways in which information can be used rapidly across sectors for decision making. For example, water storage may be necessary if piped water is not available, not consistent, or the quality is poor; piles of discarded items may be found on premises or in informal dumping areas if households and businesses do not have access routine trash collection services; and tires may be found on premises or in informal dumping areas even when regular trash collection exists, because they are generally not collected (tires cannot be placed in landfills, and there are few facilities incinerate or recycle them). During an epidemic, hotels may incur high costs spray the surrounding area keep the adult mosquito population down, and shortages in staff due illness may affect tourist-dependent businesses, both in levels of service provided and tourists perceptions of the quality of service. In addition, advocacy and intersectoral actions at the local level may help municipal and state health departments manage a broad-based program over time because of intersectoral participation from schools, businesses, churches, service organizations, social clubs, and other groups. Given that the mosquito vector lives in and around the domestic setting, laying her eggs in water-holding containers that residents have created, an understanding of the specific behaviors that lead mosquito production must be developed. The lack of even the most basic formative research for any community-related activity has resulted in the ongoing promotion of control methods that are either irrelevant and impossible sustain or ineffective in preventing mosquito production. Traditionally, dengue control programs have not used behavioral outcomes measure the impact of program activities at the household/individual level. In the case of vector control activities, general entomological indices, such as the house, Breteau, and container, are used determine whether homeowners are implementing mosquito prevention actions for containers found in and around the home. Since these indices are based on the presence of one or more larvae in a container, with no distinction between large or small numbers of larvae in the container, the indices are not sensitive enough reflect implementation of the recommended behavior. For example, a common message is that householders should empty the water from containers when they see larvae in the water. Although a householder may routinely inspect and empty the water from containers that have larvae, vector control staff conducting a house visit have continued identify a small number of larvae in the early stages of development, which can be hard see. This household would then be classified as a positive house, although the reality is that once the larvae are large enough be easily seen, the householder will empty the water. While most programs use various combinations of health education, communication, and social mobilization strategies carry out dengue prevention and control activities, integration of the strategies achieve this over the long term have not been part of community-based planning for dengue prevention and control. The lack of appropriate outcome indicators evaluate behavior changes in any of the elements of a dengue prevention and control program limits the ability of programs monitor and evaluate effectiveness of the strategies being used. Some of the best practices presented in Section 3 will demonstrate a mix of the above-mentioned strategies, determined by local social, cultural, financial, and political factors. Environmental management provides a flexible framework through which a wide variety of actions can be undertaken in an integrated and coherent fashion. Those same surveys have revealed, however, that residents are concerned about mosquitoes because of the pest factor and those concerns would be sufficient motivate a certain level of behavior change (Rosenbaum, et al. Yet most dengue control programs continue function under the assumption that providing more information will motivate behavior change; date, this has not occurred in a sustainable fashion. Residents desire for clean water can facilitate water storage behaviors that are favorable preventing mosquito breeding. A broader environmental management approach also paves the way for greater intersectoral collaboration through advocacy and reduction in duplication of efforts. The rapid reporting of suspected cases and the submission of blood samples taken at the appropriate times and sent in good condition the laboratory depend upon trained and informed health care professionals. Health institutions such as hospitals and clinics must then be prepared for an increase in the number of patients and, during an emergency, the management of an influx of very large numbers of patients. Dissemination of this information in a timely fashion intersectoral groups such as a dengue commission can then guide decisions intensify routine control actions or implement an emergency response using data rather than responding political pressure. Clinical surveillance should at minimum be based upon a passive surveillance system, with an active surveillance system, as described earlier, a goal work toward. A national laboratory service that can perform, at minimum, basic diagnostic tests. Incorporation of the subject of dengue and health into formal education systems School-based education programs are believed be the single best way inculcate future generations of homeowners with a sense of responsibility for environmental management. However, few vector control programs have been able sustain school-based activities due, in part, academic requirements that have led a full curriculum. Development of curricula in partnership with curriculum specialists from the Ministry of Education should go a long way toward increasing acceptance of health curricula by teachers and principals. Critical analysis of the use and function of insecticides Most national dengue prevention and control programs rely on the use of various insecticides control larval and adult stages of Ae. Typically, program budgets allocate most funds staff salaries, the purchase of chemicals, and the purchase of equipment apply the chemicals. These unrealistic perceptions of the costs of the various components continue result in programs that rely on the use of chemicals given that those purchases account for a significant portion of the budget, leaving little funding available for implementation of other components of the program. The use of chemicals has an important role and function in a comprehensive, integrated dengue prevention and control program. But how, when, and where each type of chemical is used must be critically evaluated prior its use, and the norms guiding its use rigorously enforced (see Najera and Zaim, 2002).
Adults with acquired visual impairment who will become non-drivers because of decreased visual acuity extreme weight loss 081313 buy astralean. Although individuals with acquired visual impairments are legally qualified weight loss pills 901 order 40 mcg astralean otc drive until their license is up for renewal weight loss supplement xantrax purchase astralean visa, civil liability exposure exists if they continue weight loss pills all natural generic 40 mcg astralean overnight delivery drive with the knowledge that they would no longer visually qualify weight loss pills hydroxycut buy astralean 40 mcg on line drive weight loss pills 902 generic astralean 40 mcg otc, if they attempted renew their license. At such time the vehicle is no longer used for the transport of the passenger or operator that is the subject of the exemption, the exemption expires and may not be used on any replacement vehicle purchased after July 3, 2012. The owner of the vehicle which the exemption applied must return the vehicle conformance with the minimum standard of transparency within 60 days of expiration of the exemption. Although individuals with acquired visual impairments are legally qualified drive until their license is up for renewal, civil liability exposure exists, if Ophthalmology Survival Guide Page 58 they continue drive with the knowledge that they would no longer visually qualify drive, if they attempted renew their license. This standard states that the individual is legally qualified drive, until their license comes up for renewal, regardless of whether their visual acuity or visual field becomes impaired during the interval between licensing renewal. Although individuals with acquired visual impairments are legally qualified drive until their license is up for renewal, civil liability exposure exists, if they continue drive with the knowledge that they would no longer visually qualify drive, if they attempted renew their license. An auditory, computer generated voice, test can be provided or the individual can bring someone with them read the test. During the past 6 months, Ophthalmology Survival Guide Page 61 have you made any driving errors? The author would also recommend that the letter state "I am requesting that a hearing officer provide (patient name) with a behind the wheel evaluation see if he/she can acquire/maintain the privilege of operating a motor vehicle". A statement concerning whether the eye specialist feels the individual is visually competent drive 5. A statement concerning privileges, whether they be general, daylight only, or limited 6. The reporting physician is immune from any liabilities, civil or criminal, which may otherwise be incurred or imposed as a result of the report. No need worry as long as symptoms fit what you expect with the dynamics of a floating bubble. Tearing and pain after the injection is usually due the toxicity of the iodine and numbing medication. This usually improves very quickly over the course of 12-24 hours with rest, Tylenol and artificial tears. If this does not improve (in 12-24h) or gets worse in any way, call back so we can see you. If the eye is still uncomfortable or if the lens was placed for a corneal wound leak, we can arrange for you be seen tomorrow replace it or you can see a local eye care provider if you live a long distance away. Otherwise, tape the protruding end your cheek and we will arrange see you tomorrow replace it. If you can count the number of new floaters on 1 hand, we can arrange see you in the morning (per Dr. If there are more floaters than you can count or if you are having associated flashes, we should see you tonight. Early recognition and initia tion of appropriate treatment are crucial patient outcomes. Introduction Abnormalities in hemostasis, including bleeding and thrombosis, are common complications in patients with cancer and can greatly affect mor bidity and mortality (Rodriguez, 2018). Several factors can contribute the etiology of bleeding and thrombosis, including the disease process and the use of treatment modalities that may affect bleeding or coagulation. These factors include surgical procedures, chemotherapy, biotherapy, radiation therapy, central venous catheters, supportive care with colony-stimulating factors, and newer anticoagulants (Konigsbrugge, Pabinger, & Ay, 2014; Rodriguez, 2014). Several tumor-related or treatment-related factors can increase the risk for bleeding by disrupting normal hemostatic mechanisms, including alterations in platelet function or the coagulation pathway. The presence of infection, liver disease, and the high-viscosity proteins that some tumors express can each alter the coag ulation pathway, increasing the risk for bleeding (Rodriguez, 2014). The risk for bleeding increases with cancer, but certain malignancies, especially most leukemias, are associated with a higher risk than others. Acute promy elocytic leukemia carries a particularly high risk for bleeding with as many as 90% of patients developing bleeding complications (Coombs, Tavakkoli, & Tallman, 2015). These disturbances can directly affect patient morbidity and mortal ity and present complex challenges when caring for patients with cancer. Because bleeding poses dire consequences for patients, it is imperative that any management plan includes bleeding prevention. To increase sur vival rates, rapid recognition, assessment of the precipitating factors, and knowledge of the treatment of bleeding are necessary. Ongoing bleeding can affect patients quality of life by causing fatigue and weakness. The abil ity recognize early signs of bleeding and initiate interventions can dra matically improve patients quality of life and increase their potential for survival. Oncology nurses, both in ambulatory and inpatient settings, play a key role in preventing, assessing, and managing major bleeding events and should be knowledgeable about evidence-based interventions as they evolve. Incidence Bleeding, in general, can occur with any type of cancer, and there are no specifc incidence rates for this complication. However, bleeding does occur more frequently in individuals with hematologic cancers because these cancers affect the bone marrow, often resulting in thrombocyto penia?a reduction in the number of circulating platelets. Therefore, the incidence and severity of bleeding in patients with acute leukemia are greater than in patients with solid tumors. Mucin-producing adenocarcinomas, such as those of the lung, breast, stomach, pancreas, and prostate, are more prone hemostatic abnormal ities (Escobar, Henke, & Wakefeld, 2013). Malignancies with a higher incidence of bleeding include large carcinomas of the head and neck, large centrally located lung cancers, acute myeloid leukemia, and chronic myeloid leukemia (Rodriguez, 2018). Bleeding and Thrombosis 3 Risk Factors and Etiology Several factors increase the risk of bleeding in patients with cancer. Anti neoplastic therapies increase the risk for bleeding by damaging normal tis sues. Radiation therapy and steroid treatment can cause blood vessels become fragile and more prone injury. Chemotherapy and radiation can cause myelosuppression, including thrombocytopenia, which increases the risk of bleeding. Other general risk factors for bleeding in patients with can cer include fever, sepsis, infection, anticoagulant therapy, impaired platelet function, and adverse effects of medications (Rodriguez, 2014). Because of the critical role that platelets play in hemostasis and throm bosis, the platelet count is considered be the most signifcant fac tor for predicting bleeding in a patient with cancer (Rodriguez, 2018). The frst reported association between thrombocytopenia and bleeding risk occurred in 1962, when it was demonstrated that hemorrhage rarely occurred in patients with acute leukemia when the platelet count remained higher than 20,000/mm3 (Gaydos, Freirich, & Mantel, 1962). Both drug types can drastically reduce platelet aggregation, with the effects of aspirin lasting up four days after ingestion. Antibiotic use can also contribute bleeding risk by impairing platelet function. Carbenicillin, ticarcillin, and other penicillins impair the aggre gation of platelets and prolong bleeding time (Scharf, 2012). This plate let dysfunction is maximized one three days after administration and can continue for several days after the antibiotic course is completed. Other medications that suppress platelet function include phenothiazines, tricy clic antidepressants, heparins, cimetidine, thiazide diuretics, statins, plasma expanders, antihistamines, and estrogen. In addition, corticosteroids affect the gastric mucosa and impair wound healing, resulting in the skin becom ing thin, fragile, and more susceptible bleeding. Tumor growth can lead bleeding through invasion into the surround ing structures and blood vessels, as well as the bone marrow. Leukemias and lymphomas are the most common cancers associated with bone marrow inva sion. In these diseases, the malignant cells crowd out the normal cells in the marrow, leading thrombocytopenia, anemia, and neutropenia. Tumors can also erode and enter mucous membranes and cause bleeding by local tis sue disruption. Tumors that are close large blood vessels put patients at risk for a massive hemorrhage. Other risk factors for bleeding in patients with can Copyright 2018 by Oncology Nursing Society. Viruses can cause myelosuppression or throm bocytopenia, and fungal infections, especially in the lungs, can cause fatal hemorrhage (Nucci, Nouer, Cappone, & Anaissie, 2013). Vitamin K is necessary for proper coagulation and is absorbed solely from the diet. Malnutrition can lead an increased risk of bleeding because of a vitamin K defciency, which can develop as a direct result of a dietary defciency, biliary obstruc tion, malabsorption syndromes, liver disease, and anticoagulation therapy (Nguyen-Khoa, Patel, & Mikhail, 2015). Uremic bleeding is related platelet dysfunction, including a reduced platelet count and increased plate let turnover. Uremic toxins, increased production of nitric oxide, prostacy clin, calcium, and cyclic adenosine monophosphate, along with renal anemia, cause these symptoms (Berns & Coutre, 2017). Excessive bleeding due uremia may also manifest as cardiovas cular and neurologic defcits (Alper, Shenava, & Young, 2017). Pathophysiology Normal control of bleeding (hemostasis) is maintained through a fnely regulated balance between clot formation (coagulation) and clot dissolu tion (fbrinolysis). The presence of malignancy disrupts this essential balance and can lead bleeding through several different mechanisms, including alterations in platelet count and function, activation of the coagulation cascade, disruption in vascular integrity, and the effects of antineoplastic therapies. Patients with cancer often have more than one of these conditions occurring simultane ously, putting them at increased risk for bleeding (Rodriguez, 2018). Local anatomic causes of bleeding include tumor extension and invasion of blood vessels, whereas systemic causes include bone marrow invasion by tumor cells, bone marrow suppression from chemotherapy or radiation, Copyright 2018 by Oncology Nursing Society. Factors Contributing Bleeding in Patients With Cancer Type Factors Anatomic factors Local tumor invasion Tumor involvement of vascular tissue Tumor location near major vessels Head and neck tumors Systemic factors Bone marrow involvement by tumor Bone marrow suppression Concomitant disease. Platelets and Thrombocytopenia Platelets play a crucial role in the process of hemostasis. Platelets are not true cells, but rather fragments of megakaryocytes, giant cells within the bone marrow integral the production of platelets. In the event of an injury or cut that breaks the endothelial layer of a blood vessel, platelets function as frst responders form a clot that seals the injury site and inhibits blood loss (Monroe & Hoffman, 2014). Disorders of platelet function and platelet abnormalities can affect the clotting process and put an individual at risk for severe and possibly fatal bleeding. Thrombocytopenia is the platelet abnormality most frequently associ ated with cancer. When a large bur den of tumor cells overwhelms the normal elements of bone marrow, the resulting thrombocytopenia refects an overall pancytopenia in which all cell lines are reduced. The occurrence and severity of treatment-associated thrombocytopenia depend on the type of chemotherapy drugs, dosage, and the time between treatments. With radiation therapy, the development of thrombocytopenia depends on the amount of bone marrow encompassed in the treatment felds. The development of thrombocytopenia may be a dose-limiting factor in delivering these treatments and can lead a bleed ing event (Rodriguez, 2018). Thrombocytopenia may arise indirectly in patients with cancer whose spleens have enlarged because of infection, infammation, autoimmune disor der, or neoplasm within the spleen. Splenic pooling of platelets has been iden tifed as a cause of thrombocytopenia, with approximately one-third of trans fused platelets being removed from circulation and sequestered in the spleen (Izak & Bussel, 2014). Splenic enlargement may occur with metastasis the spleen from cancers of the lung, breast, colon, prostate, and stomach, as well as lymphomas. If the spleen is not enlarged, it is unlikely that existing thrombocy topenia is the result of splenic trapping of platelets (Rodriguez, 2018). Imma ture platelets accumulate in the bone marrow while the number of circulating mature platelets diminishes. This presentation most often occurs in patients with lymphomas and may precede clinical diagnosis (Rodriguez, 2018). Platelet Refractoriness Platelet refractoriness exists when the platelet level does not increase the desired level following a platelet transfusion. It is defned as a one-hour post-transfusion platelet count that fails increase by an increment of 11,000/mm3 on two consecutive transfusions (Fletcher, DomBourian, & Millward, 2015). Platelet refractoriness has been reported in 30%?50% of patients who receive platelet transfusions (Valsami, Dimitroulis, Gialer aki, Chimonidou, & Politou, 2015). Fever, one of the most frequently cited causes, most likely is not an independent factor but rather is associ ated with underlying infection or sepsis. Splenomegaly is a well-established cause of poor response platelet transfusion. Bleeding and Thrombosis 7 which is in equilibrium the circulating platelet pool. In extreme spleno megaly, up 90% of the platelets can be sequestered (Wang et al. Immune: Refractoriness platelet transfusion caused by an immune response is known as alloimmunization and has the greatest potential for pre vention and management. To coun teract this effect, transfusions of leukoreduced platelets, in which the white blood cells (leukocytes) have been removed from the blood product, can be used decrease the potential for alloimmunization. Clotting Factor Defciencies Clotting factors are the blood components responsible for conversion of fbrinogen fbrin, which is needed form a clot. Clotting factor defcien cies can contribute bleeding risk and may occur with certain cancers. The liver also clears fbrin degradation products and acti vated clotting factors from circulation. Therefore, patients with can cer who undergo extensive surgical procedures and receive large amounts of fresh frozen plasma may become prone increased bleeding (Rodriguez, 2018). This is associated with impaired pro coagulant activities and abnormal platelet function because of alterations in platelet size, shape, and aggregation responses (Rodriguez, 2018). Clinical Manifestations Bleeding manifests in several ways in patients with cancer. Signs of bleed ing without visible hemorrhage include petechiae, ecchymoses, and bruis ing. This type of bleeding may often be overlooked because it is not thought Copyright 2018 by Oncology Nursing Society.
Buy astralean with a visa. weight loss tea without milk dairy free tea soya tea.