Prograf
Teresa M. Bieker, MBA-H, RDMS, RDCS, RVT
- Lead Sonographer
- Division of Ultrasound
- University of Colorado Hospital
- Aurora, Colorado
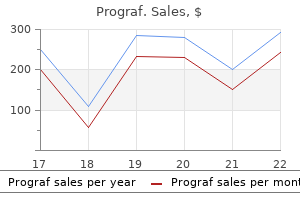
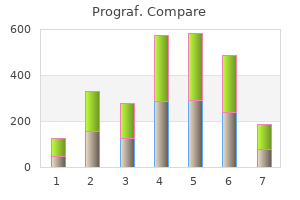
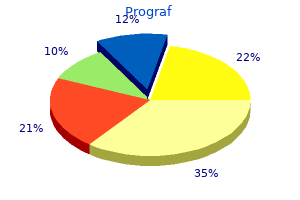
The impact of these infections on mortality natural anti viral foods buy prograf 1 mg line, length -4$T of stay and cost is outlined in Figure 8 antiviral used to treat parkinson's buy genuine prograf on line. The need to articulate clear goals and their emphasis Booklet on antimicrobial stewardship in the depending on the target audience is also important hiv infection timeline symptoms generic prograf 0.5mg line. An easy pocket guide to these priniciples as well as implementation are also available antiviral used for parkinson's discount 1 mg prograf otc. The video runs for 10 minutes and shows the response to the outbreak by the hospital team hiv infection rates 2015 prograf 0.5mg fast delivery. Think particularly about how they tried to engage clinicians and their attempts at measuring compliance with good practice hiv infection rate in kenya purchase 1 mg prograf with visa. The prescribing issues that may be worthy of investigation and the strengths and weaknesses of the response to the outbreak. This increase has antibiotic) use been greater in low and middle-income countries. This increase has been o European Surveillance of antimicrobial Consumption driven by factors such as economic growth and increased access Network to antibiotics. Percentage change in antibiotic consumption per capita 2000-2010 Center for Disease Dynamics, Economics & Policy. Between 2000-2010 their usage Interactive Map on antibiotic consumption at a increased by around 40% as did carbapenems, a reserve group country and global level. Prescribers In Europe, Australia and Canada general practitioners prescribe the majority of antibiotics in the community, dentists account for 3 -10% and nurses and other health professionals < 6%. Whilst penicillins are the most frequently used antibiotics with 30 Use in the community is highest in the very young (0-9 years) to 60% of use, the pattern of use of other antibiotic groups varies and the elderly (65+ years). For example, cephalosporins Common indications for use in the community and other beta lactams (including carbapenems) account for In developed countries, the majority of the use of antibiotics in 0. Non leading to increased use of broad spectrum agents or prescription use: unnecessary prescription of antibiotics. Health professionals are often reluctant to question prescribing decisions of colleagues and in some sectors, such as private hospitals, senior prescribers have complete autonomy in deciding what antibiotic to use, how much to use and for how long. Canadian Antimicrobial Resistance Surveillance System Report 2016 Center for Diseases Control. Discuss possible unintended consequences of In this YouTube video animation you will: antimicrobial stewardship. Within 6 days she was admitted to the hospital in septic shock where she was diagnosed with severe Clostridium difcile colitis complicated with a toxic megacolon requiring total colectomy. All cultures from blood an abdomen grew In chapter 1 you learnt about the overall clinical, microbial Klebsiella pneumoniae: and economic impact of infections with drug resistant bacteria. Antibiotic resistance not only happens in acute hospitalised patients but can start in the community. In this case, an antibiotic prescribed in the outpatient setting by a dentist lead to signifcant complications and possible mortality. Unfortunately, this is not science fction, or a new unknown infection from an exotic land. Unfortunately, the appropriate and inappropriate use of these drugs has consequences. As global rates of antibiotic resistant infections increase antibiotic research and development has been dwindling, resulting in a catastrophic lack of weapons to use in this public health crisis. In response to this challenge, healthcare workers on the front lines have been tasked with minimizing unnecessary and inappropriate prescribing of antibiotics in order to prevent development of resistance while maintaining or improving patient outcomes. Figure 3 provides more detail to each principle as relates it to clinical evaluation. One of the goals of antimicrobial stewardship is to minimise or prevent unnecessary changes in the gut biome to prevent the development and transmission of antimicrobial resistance among our commensal biome. Antimicrobial stewardship programs have a direct responsibility to ensure prudent antibiotic prescribing. Inadequate initiation of antibiotics can Antibiotics Cause prolonged alterations to Gut Microbiome increase mortality by up to 50%. These clinical pathways can either be built into the medical record software at the time of prescribing, or can be available to prescribers via a manual or internet portal. Timely de-escalation (being part of the review of antibiotic prescriptions) will minimize patient exposure to broad spectrum antimicrobials and therefore reduce their risk for associated events such as resistance or C. Surgical site In addition, prolonged courses of antibiotics increase the risk of infections are among the most common healthcare-associated colonisation with multidrug resistant organisms. Therefore, the infections globally and have been associated with increased chain of transmission (in particular within healthcare settings) post-operative hospital days, additional surgical procedures, increases the risk of horizontally infecting more than one and often higher mortality. Europe has seen a statistically signifcant decrease in surgical site infections between 2009 and 2012 in the areas of cesarean section (p<0. In common cost outcomes evaluated in stewardship studies hospitals and long-term care facilities, C. De-escalation Total cost savings of In order to reduce antibiotic consumption and costs without $38,920. Computerized Savings of 84,188 monitoring software compared to control access to rapid diagnostic options. These core elements are as commit ourselves to using these precious resources wisely. Ensuring that patients However, a successful program requires the involvement of well are started on the correct guideline-based therapy can prevent trained and enthusiastic physicians and pharmacists and the further fuoroquinolone resistance from developing due to strong support of the healthcare administration and medical staf. Three sets of blood cultures unintended consequences that should be tracked and reported are taken and patient is empirically started on vancomycin and concurrently with the primary outcomes. Discontinue cefepime and vancomycin, initiate ceftaroline prophylaxis infections d. Am J Nonetheless, balancing measures to detect unintended negative Surg, 189(4), 395. Guidelines for Balancing measures (looking at a system from diferent diagnosis, treatment, and prevention of clostridium difcile infections. These can be as basic or as complex barriers to these stages and as resources allow a range of relatively simple interventions can produce measurable suggest solutions to changes in antimicrobial use, but if the ultimate aim is to drive improvements in the quality overcome them. If it is length of stay consumption of of infections due to a stand-alone group, it should be integrated into the governance broad spectrum key multi-resistant structure of the organisation so that it is accountable. The antibiotics organisms diagram below outlines how such a committee might ft in a this business case should outline any initial and ongoing hospital setting. Even a limited stewardship setting, and the diagram below lists some, but is not exhaustive. The table below provides examples Critical incidents/patient safety issues of stewardship activities that may be relevant, with an organisation may have reporting system for patient safety approximation of the timescales involved in implementing any incidents; monitor for incidents relating to antimicrobial use; activity and the level of input required to implement and maintain audits of door to needle times for sepsis; high rate of surgical site it going forward. In such situations, the time and efort required to develop guidelines from scratch may be considerable, and it may be Developing educational resources can be challenging, especially a more cost-efective initial step to borrow and adapt other in resource limited settings. Once this is done, there should be a plan to review these on a regular basis to ensure that they remain relevant and current. For pharmacy professionals, they may also be required to provide general clinical pharmacy services on wards or in the pharmacy department. In reality, there are always a number of barriers to educational events or courses by-theme-initiative/ implementing any programme and these vary depending on the for key staf healthcare-associated local situation. The table below lists the most Health Education England commonly reported barriers. See chapter 13 for more information on education and competencies, including examples from other countries. But perhaps with a specifc resource or structural modifcation, even more remarkable things could be accomplished! If so, take heart: that is an opportunity for change, and you may be the one to take the lead. But, if the level of patient complexity Certainly, funding is an important consideration. Micro lab directors can provide antibiotic resistance data, guide providers at the point of care with savvy messaging, and implement rapid diagnostic testing to facilitate prompt de escalation of empiric therapy. Nurses and Clinical Ofcers are front-line partners in care, and may have a large impact upon the success or failure of stewardship programs. These activities require expertise, and asking the stewardship leaders to take this on may "Pharmaceutical (296)" fickr photo by Doug Waldron negatively impact their productivity. Finally, is there assistance for the stewards in arranging meetings, Efective stewardship programs are led by pharmacists and tracking projects, and staying organised In large centres, stewardship may be a full-time job, whereas in smaller hospitals a reduced fraction of efort may be appropriate. But, because clinical medicine requires tremendous time and energy, these questions require clear answers: Will stewardship leaders be paid for their time, or will they have to apply for grants to support their wages The ideal ratio of stewards to patients is uncertain, and likely depends on the setting (for example, inpatient versus ambulatory). If the pharmacist expects the physician to review every intervention, then progress may be painfully slow. This relationship should be structured in the most equitable and efcient way possible. Will the stewards be nested within the infection prevention team, or will they be considered a separate entity The pharmacist and physician stewardship leaders should know precisely what their supervisors want and expect to "Health and Medical Cloud" fickr photo by perspec photo88 hear regarding progress and impact. Executive sponsors need to know that they are getting a good return on their investment, so they may focus Does your centre embrace computerised order entry If so, does it track are set, the stewards should know what the implications are if antibiotic orders or actual administrations, for instance via they are missed. Most programs employ a combination of prospective audit with feedback and formulary restriction. Written recommendations may improve recommendation acceptance, but getting those notes into the chart takes time. If a separate infectious diseases consultant practices in the hospital, is that person informed of recommendations being made by the stewardship team, to ensure a coordinated efort and consistent messaging Is time allotted One daily activity model emphasises formulary restriction, in for data abstraction, analysis, and presentation This approach has been demonstrated be reviewed for consideration of addition to the formulary Guideline Compliance If the stewardship team has published guidelines for antimicrobial use, or created order sets for common infections, how frequently are they being followed A related metric is time to efective therapy: How long does it take teams to get their septic patients onto the appropriate antimicrobial spectrum Even one of these events will harm the patient the drug in question is considered a day of therapy. The greatest measure of motivation is a demonstrated commitment to efective antimicrobial stewardship. Stewardship Program: Guidelines by the Infectious Diseases Society of America and the Society for 3. National Quality Forum, National Quality Partners, Antibiotic Stewardship Action Team. Guidance for the knowledge and skills required for antimicrobial stewardship leaders. You may need to look at other resources or talk to others within or outside of your organisation to fll in the gaps once you have had a go. Whilst these programmes may be aligned at strategic level, this alignment does not always transfer to the day to day operational life of the organisation. Those countries which have a strategy in place will be there are limited published examples and almost all are from thinking about execution and implementation. This does not mean that such models asks you to extend the assessments made above to your own do not exist in low and middle income countries, but that they national action plan. Readers are encouraged to also look at have not been shared in the international literature.
Licensing of new quercetin antiviral activity generic 1 mg prograf fast delivery, improved hiv infection circumcision order prograf 0.5 mg amex, and safer vaccines; anticipated arrival of additional combination vaccines; establishment of an adolescent immunization platform; and application of novel vaccine-delivery systems promise a new era of preventive medicine hiv infection treatment guidelines order prograf 0.5mg visa. The advent of population-based postlicensure studies of new vaccines facilitates detection of rare adverse events temporally associated with immunization that were undetected during prelicensure clinical trials hiv infection rate in uae cheap 1mg prograf with amex. Identifcation of the rare occurrence of intussusception after administration of the frst licensed oral rhesus rotavirus vaccine confrmed the value of such surveillance systems historical hiv infection rates order prograf 0.5 mg overnight delivery. Physicians must regularly update their knowledge about specifc vaccines hiv infection treatment prograf 0.5mg with mastercard, including information about their recommended use, safety, and effectiveness. Each edition of the Red Book provides recommendations for immunization of infants, children, and adolescents. Whereas immuni zation recommendations represent the best approach to disease prevention on a population basis, in rare circumstances, individual considerations may warrant a different approach. Comparison of 20th Century Annual Morbidity and Current Morbidity: Vaccine-Preventable Diseasesa 20th Century 2010 Reported Percent Disease Annual Morbidityb Casesc Decrease Smallpox 29 005 0 100 Diphtheria 21 053 0 100 Measles 530 217 63 >99 Mumps 162 344 2612 98 Pertussis 200 752 27 550 86 Polio (paralytic) 16 316 0 100 Rubella 47 745 5 >99 Congenital rubella syndrome 152 0 100 Tetanus 580 26 96 Haemophilus infuenzae 20 000 246d 99 a National Center for Immunization and Respiratory Diseases. Comparison of Prevaccine Era Estimated Annual Morbidity With Current Estimates: Vaccine-Preventable Diseasesa Prevaccine Era 2010 Reported Disease Annual Estimate Cases Percent Decrease Hepatitis A 117 333b 9670c 92 Hepatitis B (acute) 66 232b 3374c 95 Pneumococcus (invasive) All ages 63 067b 16 569c 84 <5 years of age 16 069b 1877c 88 Rotavirus (hospitalizations, 62 500d 28 125e 55 <3 years of age) Varicella 4 085 120b 9920c 99. Historical comparisons of morbidity and mortality for vaccine-preventable diseases in the United States. Sources of Vaccine Information In addition to the Red Book, which is published every 3 years, physicians should use evidence-based literature and other sources for data to answer specifc vaccine questions encountered in practice. Each product insert lists contents of the vaccine, including preservatives, stabilizers, antimicrobial agents, adjuvants, and suspending fuids. Health care professionals should be familiar with the label for each product they administer. Most manufacturers maintain Web sites with current information concerning new vaccine releases and changes in labeling. The monograph also provides information about other vaccines recommended for travel in specifc areas and other information for travelers. For additional sources of information on international travel, see International Travel (p 103). Annual course offerings include the Immunization Update, Vaccines for International Travel, Infuenza, and a 9-module introductory course on the Epidemiology and Prevention of Vaccine-Preventable Diseases. The course schedule, slide sets, and written materials can be accessed online ( This system responds to immunization-related questions submitted from health care profession als and members of the public. The hotline is a telephone-based resource available to answer immunization-related questions from health care professionals and members of the public. Appendix I (p 883) provides a list of reliable immunization information resources, including facts concern ing vaccine effcacy, clinical applications, schedules, and unbiased information about safety. Two resources comprehensively address concerns of practicing physicians: the National Network for Immunization Information ( Information can be obtained from state and local health depart ments about current epidemiology of diseases; immunization recommendations; legal requirements; public health policies; and nursery school, child care, and school health concerns or requirements. Information regarding global health matters can be obtained from the World Health Organization ( Online catch-up immunization schedulers are available for use by parents, other care providers, and health care professionals. The schedulers are based on the recommended immunization schedules for children, adolescents, and adults. The schedulers, which can be downloaded, allow the user to determine vaccines needed by age and are useful for viewing missed or skipped vaccines quickly accord ing to the recommended childhood and adult immunization schedules. The inter active vaccine schedules are available at the following sites: catch-up scheduler. Questions should be encouraged, and adequate time should be allowed so that information is understood ( This applies in all settings, including clinics, offces, hospitals (eg, for the birth dose of hepatitis B vaccine), and pharmacies. Health care professionals also should be aware of local confdentiality laws involving adolescents. Health care professionals should be familiar with requirements of the state in which they practice. Parental Concerns About Immunization Health care professionals should anticipate that some parents will question the need for or the safety of immunizations, want to space out vaccines, refuse certain vaccines, or even decide to reject all immunizations for their child. Some parents may have religious or philosophic objections to immunization, which are permitted by some states. Several factors contribute to parental vaccine concerns or lack of understanding of the benefts of vaccines, including: (1) lack of infor mation about the vaccine being given and about immunizations in general; (2) opposing information from other sources (eg, alternative medicine practitioners, antivaccination organizations, some religious groups, and alternative Web sites); (3) mistrust of the source of information (eg, vaccine manufacturer); (4) perceived risk of serious vaccine adverse events; (5) concern regarding number of injections or the vaccine schedule; (6) informa tion being delivered in a way that does not recognize cultural differences or that is not tailored to individual concern; (7) information being delivered at an inconvenient time; (8) not perceiving risk of vaccines accurately; and (9) lack of appreciation of the sever ity of vaccine-preventable diseases. One important aspect physicians can control is their relationship with patients and their parents. A non judgmental approach is best for parents who question the need for immunizations. Ideally, health care professionals should determine in general terms what parents understand about vaccines their children will be receiving, the nature of their concerns, their health beliefs, and what information they fnd credible. People understand and react to vaccine information on the basis of a variety of factors, including previous experiences, attitudes, health beliefs, personal values, and education. For some people, the risk of immunization can be viewed as disproportionately greater than the risk of disease so that immunization is not perceived as benefcial, in part because of the relative infre quency of vaccine-preventable diseases in the United States. Others can dwell on socio political issues, such as mandatory immunization, informed consent, and the primacy of individual rights over that of societal beneft. Parents may be aware through the media or information from alternative Web sites about alleged controversial issues concerning vaccines their child is scheduled to receive. When a parent initiates discussion about an alleged vaccine controversy, the health care professional should listen carefully and then calmly and non judgmentally discuss specifc concerns. Health care professionals always should provide factual information and use language appropriate for parents and other care providers. Through direct dialogue with parents and use of available resources, health care profes sionals can help reduce and possibly prevent acceptance of inaccurate media reports and information from nonauthoritative sources. Encouraging a dialogue may be the most important step to eventual vaccine acceptance. Parents who refuse vaccines should be advised of state laws pertaining to school or child care entry, which can require that unimmunized children not attend school during disease outbreaks. This informed refusal documentation should note that the parent was informed why the immunization was recommended, the risks and benefts of immunization, and the possible consequences of not allowing the vaccine to be administered. Parental Refusal of Immunization the approach of a health care professional to a parent who refuses immunization of his or her child is complex and should be based on the reason for refusal and knowledge of the parent. Pediatricians and nurses should discuss benefts and risks of each vaccine, because a parent who is reluctant to accept administration of 1 vaccine may be willing to accept others. Only then should state agencies be involved to override parental discretion on the basis of medical neglect. Active Immunization Active immunization involves administration of all or part of a microorganism or a modi fed product of a microorganism (eg, a toxoid, a purifed antigen, or an antigen produced by genetic engineering) to evoke an immunologic response that mimics that of natural infection but usually presents little or no risk to the recipient. Immunization can result in antitoxin, anti-adherence, anti-invasive, or neutralizing activity or other types of pro tective humoral or cellular responses in the recipient. Some immunizing agents provide nearly complete and lifelong protection against disease, some provide partial protection, and some must be readministered at regular intervals to maintain protection. The immu nologic response to vaccination is dependent on the type and dose of antigen, the effect of adjuvants and host factors related to age, preexisting antibody, nutrition, concurrent disease, or drug effect and genetics of the host. The effectiveness of a vaccine is assessed by evidence of protection against the natural disease. Vaccines incorporating an intact infectious agent may contain live-attenuated, inactivated, or genetically engineered subunits. Among currently licensed vac cines in the United States, there are 2 live-attenuated bacterial vaccines (oral typhoid and bacille-Calmette Guerin vaccines) and several live-attenuated viral vaccines. Although active replication (with bacterial or viral replication) ensues after administration of these vaccines, infection is modifed, and little or no adverse host effect is expected. Vaccines for some viruses (eg, hepatitis A and hepatitis B, human papillomavirus) and most bacteria are inactivated, component, subunit (purifed components) preparations or inactivated toxins. Some vaccines contain purifed bacterial polysaccharides conjugated chemically to immunobiologically active proteins (eg, tetanus toxoid, nontoxic variant of mutant diphtheria toxin, meningococcal outer membrane protein complex). Viruses and bacteria in inactivated, subunit, and conjugate vaccine preparations are not capable of replicat ing in the host; therefore, these vaccines must contain a suffcient antigen content to stimulate a desired response. In the case of conjugate polysaccharide vaccines, the protein linkage between the polysaccharide and the protein enhances vaccine immuno genicity. Maintenance of long-lasting immunity with inactivated viral or bacterial vaccines and toxoid vaccines may require periodic administration of booster doses. Although inacti vated vaccines may not elicit the range of immunologic response provided by live-atten uated agents, effcacy of licensed inactivated vaccines is high. For example, an injected inactivated viral vaccine may evoke suffcient serum antibody or cell-mediated immunity but evoke only minimal mucosal antibody in the form of secretory immunoglobulin (Ig) A. Mucosal protection after administration of inactivated vaccines generally is inferior to mucosal immunity induced by live-attenuated vaccines. Nonetheless, the demonstrated effcacy for such vaccines against invasive infection is high. Bacterial polysaccharide con jugate vaccines (eg, Haemophilus infuenzae type b and pneumococcal conjugate vaccines) reduce nasopharyngeal colonization through exudated IgG. Viruses and bacteria in inac tivated vaccines cannot replicate in or be excreted by the vaccine recipient as infectious agents and, thus, do not present the same safety concerns for immunosuppressed vaccin ees or contacts of vaccinees as might live-attenuated vaccines. Recommendations for dose, vaccine storage and handling (see Vaccine Handling and Storage, p 16), route and technique of administration (see Vaccine Administration, p 20), and immunization schedules should be followed for predictable, effective immunization (see also disease-specifc chapters in Section 3). Adherence to recommended guidelines is criti cal to the success of immunization practices. Major constitu ents, including cell line derivation or animal derivatives, as relevant, are listed in package inserts. Sometimes multiple vaccines, each made by a different manufacturer, are licensed for similar indications and use. When this is the case, physicians should be aware that such products may have different active and/or inert ingredients. Some vaccines consist of a single antigen that is a highly defned constituent (eg, tetanus or diphtheria toxoid). Other vaccines consist of multiple antigens, which can vary substantially in chemical composition and number (eg, acellular pertussis components, Haemophilus infuenzae type b, and pneu mococcal and meningococcal products). Carrier proteins of proven immunologic potential (eg, tetanus toxoid, nontoxic variant of diphtheria toxin, meningococcal outer membrane pro tein complex), when chemically bound to less immunogenic polysaccharide antigens (eg, H infuenzae type b, meningococcal and pneumococcal polysaccharides), enhance the type and magnitude of immune responses, particularly in children younger than 2 years of age, who have immature immune systems. Sterile water for injection or saline solution is used commonly as a vaccine vehicle or suspending fuid. Some vaccine products use a complex tissue culture fuid, which may contain proteins or other constituents derived from the medium and biological system in which the vaccine is produced (eg, egg antigens, gelatin, or cell culture-derived antigens). Some vaccines and immune globulin preparations contain added substances (eg, preservatives or stabi lizers) or residual materials from the manufacturing process (eg, antibiotic agents or other chemicals, including trace amounts of thimerosal). Allergic reactions may occur if the recipient is sensitive to one or more of these additives. Whenever feasible, these reactions should be anticipated by screening the potential vaccinee for known severe allergy to specifc vaccine components. Standardized forms are available to assist clini cians in screening for allergies and other potential contraindications to immunization ( Thimerosal has been the most commonly used preservative in vac cines, added to multidose vaccine vials specifcally to kill or inhibit growth of micro organisms. All routinely recommended vaccines for infants and children in the United States are available only as thimerosal-free formulations or contain only trace amounts of thimerosal, with the exception of some inactivated infuenza vaccines. Institute of Medicine safety reviews regarding thimerosal-containing vaccines as well as vaccines and autism are available 1 ( An aluminum salt commonly is used in varying amounts to increase immu nogenicity and to prolong the stimulatory effect, particularly for vaccines containing inactivated microorganisms or their products (eg, hepatitis B vaccine and diphtheria and tetanus toxoids). Vaccine Handling and Storage Vaccines should be transported and stored at recommended temperatures. Inattention to vaccine handling and storage conditions can contribute to vaccine failure. Inactivated vaccines may tolerate limited exposure to elevated temperatures but are damaged rapidly by freezing (cold sensitive).
This restriction also applies to over the-top applications in roundup ready corn and cotton hiv infection early signs and symptoms purchase prograf visa. Aerial Equipment Use the directed rates of this product in 3 to 15 gallons of water per acre antiviral quizlet discount prograf 0.5mg otc. Use the following guidelines when aerial applications are made near crops or desirable perennial vegetation after bud break and before total leaf drop antiviral for shingles trusted 1 mg prograf, and/or near other desirable vegetation or annual crops hiv infection rate hong kong order prograf 0.5mg. For Aerial Application is Fresno County anti viral pneumonia buy generic prograf pills, California Only From February 15 Through March 31 Only hiv infection treatment buy prograf 5mg on-line. Applicable Area: the area contained inside the following boundaries within Fresno County, California. Observe the following directions to minimize off-site movement during aerial application of this product. Minimization of off-site movement is the responsibility of the grower, Pest Control Advisor and aerial applicator. All aircraft must be inspected, critiqued in flight and certified at a Fresno County Agricultural Commissioner approved fly-in. Test and calibrate spray equipment at intervals sufficient to insure that proper rates of herbicides and adjuvants are being applied during commercial use. Demonstration of performance at Fresno County Agricultural Commissioner approved fly-ins constitutes such documentation, or other written records showing calculations and measurements of flight and spray parameters acceptable to the Fresno County Agricultural Commissioner. Note: For aerial application from April 1 through February 14, refer to the For Aerial Application in California Only section of this label. Use sufficient carrier volume and appropriate equipment set-up to form droplets large enough to avoid drift potential. Applications must typically be made with the nozzle release point at 8 to 15 feet above the top of the target plants unless a greater height is required for aircraft safety. The distance of the outermost nozzles on the boom must not exceed 75% of the length of the wingspan or rotor. In many cases, reducing this distance to 65% of the length of the wingspan or rotor will improve drift control without affecting the swath width. Nozzles must always discharge backward parallel with the air stream and never discharge downwards more than 45 degrees on fixed wing aircraft or forward of the prevailing airflow on rotary winged aircraft. Do not apply when there is a low-level inversion where fine spray particles could be suspended in still air and move outside the target area when the inversion layer moves. Use the following guidelines when applications are made near crops or other desirable vegetation: 1. If wind up to 5 miles per hour is blowing toward desirable vegetation or crops, do not apply within 500 feet upwind of the desirable vegetation or crops. Winds blowing from 5 to 10 miles per hour toward desirable vegetation or crops will likely require buffer zones in excess of 500 feet. As density of weeds increases, spray volume must be increased within the directed range to ensure complete coverage. For applications made on a spray-to-wet basis, spray coverage must be uniform and complete. For annual weeds over 6 inches tall, or unless otherwise specified, use a 1 percent solution. For best results, use a 2 percent solution on harder-to-control perennials, such as bermudagrass, dock, field bindweed, hemp dogbane, milkweed and Canada thistle. When using application methods which result in less than complete coverage, use a 5 percent solution for annual and perennial weeds and a 5 to 10 percent solution for woody brush and trees. In cropping systems, a hooded sprayer, shielded sprayer, or wiper applicator may be used in-between rows of crop plants (row middles). A wiper applicator may be used over the top of crops only when specifically directed on this label. Selective equipment must be capable of preventing all contact of the herbicide solutions with the crop and operated without spray-mist escape, leakage, or dripping of the herbicide solution onto the crop. Contact of the herbicide solution with desirable vegetation may result in damage or destruction. Applicators used above desirable vegetation must be adjusted so that the lowest spray stream or wiper contact point is at least 2 inches above the desirable vegetation. Droplets, mist, foam or splatter of the herbicide solution settling on desirable vegetation may result in discoloration, stunting or destruction. Applications made above the crops must be made when the weeds are a minimum of 6 inches above the desirable vegetation. This may occur in dense clumps, severe infestations or when the height of the weeds varies so that not all weeds are contacted. A hooded sprayer is a type of shielded sprayer where the spray pattern is fully enclosed, including the top, sides, front and back, thereby shielding the crop from the spray solution. When applying around crops grown on raised beds, ensure that the hood is capable of completely enclosing the spray pattern. If necessary, extend the front and rear gaps of the hooded sprayer downward to reach the ground in deep furrows. The equipment must be configured and operated in a manner that minimizes bouncing and avoids raising the hood up off the ground surface at any time. If the hood is raised, spray particles may escape and come into contact with the crop, causing damage or destruction of the crop. Avoid operating this equipment on rough or sloping terrain where the spray hood might be raised up off the ground surface. Use hood designed to minimize excessive dripping or run-off down the insides of the hood, such as single, low pressure, low-drift, flat-fan nozzle, with an 80-90 degree spray angle positioned at the top center of the hood, with a spray volume of 20-30 gallons per acre. The following procedures can reduce the potential for crop injury when using a hooded sprayer: the spray hoods must be operated on the ground or skimming across the ground surface. Crop injury may occur when foliage of treated weeds comes into direct contact with leaves of the crop. Do not apply this product when leaves of the crop are growing in direct contact with weeds to be treated. Droplets, mist, foam or splatter of the herbicide solution settling onto desirable vegetation may result in discoloration, stunting or destruction. Wiper Applicators A wiper applicator is a device that physically wipes this product directly onto the weed. Equipment must be designed, maintained and operated to prevent the herbicide solution from contacting desirable vegetation. Performance may be improved by reducing speed in areas of heavy weed infestations. Be aware that on sloping ground, the herbicide solution may migrate, causing dripping on the lower end and drying of the wicks on the upper end of the wiper applicator. Mix only the amount of solution to be used during a 1-day period, as reduced product performance may result from use of solutions held in storage. Clean wiper parts immediately after using this product by thoroughly flushing with water. For rope or sponge wick applicators Mix 1 gallon of this product in 2 gallons of water to prepare a 33 percent solution. For panel applicators solutions ranging from 33 to 100 percent of this product in water may be used in panel wiper applicators. It may be used as a liquid concentrate or diluted prior to injecting into the spray stream. Do not mix this product with the concentrate of other products when using injection systems. For the control of perennial weeds, apply a 20 to 40 percent solution of this product at a flow rate of 2 fluid ounces per minute and a walking speed of 0. Controlled droplet application equipment produces a spray pattern which is not easily visible. Extreme care must be exercised to avoid spray or drift contacting the foliage or any other green tissue of desirable vegetation, as damage or destruction may result. See the individual crop sections for specific instructions, preharvest intervals, additional precautions and restrictions. Types of Applications: Chemical fallow, Preplant fallow beds, Pre-plant, At planting, Pre-emergence, Hooded sprayers in row-middles, Shielded Sprayers in Row-Middles, Wiper applications in row-middles and Post-harvest treatments. Use Directions: Apply this product during fallow intervals preceding planting, prior to planting or transplanting, at planting, or pre-emergent to annual and perennial crops listed in this label, except where specifically limited. For any crop not listed on this label, applications must be made at least 30 days prior to planting. Hooded sprayers and wiper applicators capable of preventing all crop contact with herbicide solutions may be used in mulched or un-mulched row middles after crop establishment. Crop injury is possible with these applications and shall be the sole responsibility of the applicator. All treatments described in the sections that follow may be made using aerial application equipment where appropriate, provided that the applicator complies with the precautions and restrictions specified on this label. Calculate the application rates and ensure that the total use of this and other glyphosate or sulfosate containing products does not exceed stated maximum use rate. Precautions: Avoid contact of this herbicide with foliage, green shoots or stems, bark, exposed roots (including those emerging from plastic mulch), or fruit of crops, as severe crop injury or destruction may result. When making at-planting and preemergence applications, application must be made before crop emergence to avoid severe crop injury. Broadcast application made at emergence will result in injury or death of emerged seedlings. Apply before seed germination in 12 coarse sandy soils to further minimize the risk of injury. Unless otherwise specified on this label, treatment with selective equipment, including wiper applicators and hooded sprayers, must be made at least 14 days prior to harvest. Restriction: In crops where spot treatment is allowed, do not treat more than 10 percent of the total field to be harvested. Precaution: Take care not to spray or allow spray to drift outside the target area in order to avoid unwanted crop destruction. Do not harvest or feed treated vegetation for 8 weeks following broadcast postemergence application, unless otherwise specified. Flush fields prior to application to obtain uniform germination and stand of red rice. Make application when the majority of the red rice plants are at the 2 leaf state and no more than 4 inches tall. Precaution: Avoid spraying during conditions of low humidity, as reduced control may result. Restrictions: Do not treat rice fields or levees when the fields contain flood water. To control common rye or cereal rye, apply after the weeds have headed and achieved maximum growth. For feed barley, apply after the hard-dough stage when the grain contains 20 percent moisture or less. For wheat, apply after the hard-dough stage of grain (30% or less grain moisture). Precautions, Restrictions: Do not apply more than 1 quart of this product per acre. Preharvest application on barley or wheat grown for seed could result in a reduction in germination or vigor. Buyer and users are responsible for any and all loss or damage in connection with the preharvest use of this product on barley or wheat grown for seed. For any crop not listed on this label, applications must be made at least 30 days prior to planting the next crop. When using nitrogen solution as a carrier, application rate may need to be increased for acceptable weed control. Restrictions: In Southern states, do not apply this product in nitrogen solutions to tough-to-control grasses such as barnyardgrass, fall panicum, broadleaf signalgrass, annual ryegrass and any perennial weeds. This includes Illinois and Indiana south of Route 50, Alabama, Arkansas, Delaware, Florida, Georgia, Kentucky, Louisiana, Maryland, Mississippi, New Jersey, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, Virginia and West Virginia. Precautions, Restrictions: Corn must be at least 12 inches tall, measured without extending leaves. Do not apply more than 1 quart of this product per acre for each hooded sprayer application and no more than 3 quarts per acre per year total. Precautions, Restrictions: It is not specified that corn grown for seed be treated because a reduction in germination or vigor may occur. Buyer and all users are responsible for any and all loss or damage in connection with the preharvest use of this product on corn grown for seed. Application of this product must be made at least 30 days prior to panting any crop not listed on this label. Precautions, Restrictions: Do not treat more than 10 percent of the total field area to be harvested. Restriction: Do not apply more than 2 quarts of this product for preharvest application.
Metastases from the breast focal sinusoidal dilatation hiv infection mouth ulcers generic prograf 0.5 mg without prescription, is found in the and extrahepatic biliary tree hiv infection symptoms ppt discount prograf 5 mg without prescription, and a may be identified by the combined use of liver adjacent to space-occupying le signet-ring cell appearance suggests a zinc-2-glycoprotein symptoms of hiv infection in toddlers purchase prograf without a prescription, gross cystic dis sions antiviral drugs pdf buy prograf australia. Perhaps the easiest pat ease fluid protein 15 and oestrogen suggests the possibility of a metastatic tern to recognize as metastatic in origin receptor antiviral herbs discount prograf 1mg on-line. Metastases from the colorectum fre clinical practice are undifferentiated Prognosis quently have well defined edges where small cell carcinomas hiv transmission statistics canada order cheap prograf online, characteristically In most cases, disseminated disease is as those from other glandular sites tend producing an enlarged liver due to dif present which precludes surgical inter to be more diffuse. Due to recent improvements in tases are also frequently necrotic and tumour may still be small, asymptomatic imaging techniques, more metastatic may show calcification . Squamous cell and carcinomas are being diagnosed early, the presence of carcinoma-in-situ in adenocarcinomas will metastasize to the providing the possibility of surgical intrahepatic bile ducts in the vicinity of an liver but their existence is usually known resection in a greater number of patients. The same applies to squamous When curative resection is feasible, cholangiocarcinoma. However, this may cell carcinomas of the oesophagus and 5-year survival can be as high as 40%; be mimicked by intrabiliary ductal growth cervix. Squamous cell carcinomas of the without surgical therapy, median sur of metastatic colonic adenocarcinoma head and neck seldom involve the liver. Analysis of cytokeratin expres Neuroendocrine/islet cell/carcinoid tu expected . The incidence of gallbladder carcinoma shows prominent geographic, gender, and racial differences, while extrahepatic bile duct carcinomas show none of these varia tions. Aetiologic associations include gall stones, sclerosing cholangitis, ulcerative colitis, abnormal choledochopancreatic junction, choledochal cysts, and infestation with liver flukes. The classification applies to carcinomas of extrahepatic bile ducts and those of choledochal cysts. Sripa Definition Age and sex distribution A malignant epithelial tumour with glan Carcinomas of the gallbladder and extra dular differentiation, arising in the gall hepatic bile ducts are diseases of older bladder or extrahepatic biliary system. Gallbladder carci Epidemiology nomas have a strong female predomi Most tumours of the gallbladder and nance, whereas extrahepatic bile duct extrahepatic bile ducts are carcinomas. Aetiology Geographic distribution Unlike carcinoma of the extrahepatic bile the incidence of carcinoma of the gall ducts, gallbladder carcinomas are not bladder varies in different parts of the associated with primary sclerosing world and also differs among different cholangitis or ulcerative colitis. In the United States, carcinoma of the gall Gallbladder carcinoma bladder is more common in Native Gallstones. The incidence of gallbladder Americans and Hispanic Americans than cancer is higher in patients with gall in whites or blacks; the rate among stones than in patients without stones female Native Americans is 21 per , and stones are present in over 80% Fig. In Latin American dence of gallbladder carcinoma paral countries, the highest rates are found in lels that of gallstones, being more fre Chile, Mexico and Bolivia. In Japan, the quent in females and in certain ethnic incidence rates are intermediate. Native Americans, who general population of the United States have a high incidence of stones. While some authors have reported females in the general population of the a correlation between gallstone size and United States . Data largely reported from Japan indicate an association between gall bladder cancer and an abnormal junc tion of the pancreatic and common bile ducts . Normally, the main pancre atic duct and the common bile duct unite within the sphincter to form the pancre aticobiliary duct. The abnormal junction is defined as the union of the pancreatic and common bile ducts outside the wall of the duodenum beyond the influence of the sphincter of Oddi. Submu Carcinomas of the extrahepatic bile cosal growth is an important feature of ducts usually present relatively early with signet ring and small cell carcinomas. Jaundice usually ducts have been divided into polypoid, appears while the tumour is relatively nodular, scirrhous constricting, and dif small before widespread dissemination fusely infiltrating types. If cholangitis develops, tumours, this separation is rarely possi chills and fever appear. In patients with ble in practice because of overlapping carcinoma of the proximal bile ducts gross features. The nodular and scir plastic, and neoplastic changes in the (right and left hepatic ducts, common rhous types tend to infiltrate surrounding gallbladder epithelium. Diffuse calcifica are dilated, the gallbladder is not palpa fusely infiltrating types tend to spread lin tion of the gallbladder wall (porcelain ble and the common duct often collaps early along the ducts. The gallbladder may be distended Adenocarcinoma seem to play a role in the pathogenesis by the tumour, or collapsed due to Well to moderately differentiated adeno of carcinomas of the extrahepatic bile obstruction of the neck or cystic duct. Papillary car composed of short or long tubular glands Cancer of the gallbladder usually pres cinomas are usually sessile and exhibit a lined by cells that vary in height from low ents late in its course. Right mas have a mucoid or gelatinous cut sur quently present in the cells and glands. Carcinoma 207 Histological variants of adenocarcinoma noma with focal mucin production are Papillary adenocarcinoma. This malig usually found and are useful in separating nant tumour is composed predominantly primary from metastatic clear cell carci of papillary structures lined by cuboidal nomas. In some clear cell adenocarcino or columnar epithelial cells often contain mas of the biliary tree the columnar cells ing variable amounts of mucin. Some contain subnuclear and supranuclear tumours show intestinal differentiation vacuoles similar to those seen in secreto with collections of goblet, endocrine, and ry endometrium. Papillary adenocarcinomas tiation with production of alpha-fetopro may fill the lumen before invading the tein has been documented in clear cell Fig. In addition, skip lesions may be ing intracytoplasmic mucin displacing observed in approximately 10% of cases the nuclei toward the periphery predomi . Lateral spread through unusual variant of adenocarcinoma is the lamina propria is a common feature. Mucinous adenocarcinomas of the biliary tree are similar to those that arise in other anatomic sites. About variant is characterized by small groups one-third of the well differentiated tumours or clusters of cells surrounded by abun show focal intestinal differentiation and dant mucin. This rare been described in the extrahepatic bile malignant tumour is composed predomi ducts . Adenocarcinomas may show nantly of glycogen-rich clear cells having cribriform or angiosarcomatous patterns. Adenosquamous carcinoma this tumour consists of two malignant components, one glandular and the other squamous. Keratin pearls are often present in the squamous com ponent, and mucin is usually demonstra ble in the neoplastic glands. Squamous cell carcinoma this malignant epithelial tumour is com posed entirely of squamous cells. The epithelial ele Immunostains for cytokeratin may clarify been referred to as pleomorphic spindle ments usually predominate in the form of the diagnosis in these spindle cell cases. The mesenchymal neoplasia can be found in the metaplas polygonal cells, but foci of well-differenti component includes foci of heterologous tic squamous mucosa . Areas of squamoid differentia Cytokeratin and carcinoembryonic anti this lesion is covered in the chapter on tion may also be seen. Rarely, foci of gen are absent from the mesenchymal endocrine tumours of the gallbladder osteoclast-like multinucleated giant cells and extrahepatic bile ducts. The presence of cytokeratin in the spindle cells may help to distin Undifferentiated carcinoma guish this tumour from carcinosarcoma. Undifferentiated carcinomas are more Undifferentiated carcinoma with osteo common in the gallbladder than in the clast-like giant cells. Characteristically, tains mononuclear cells and numerous glandular structures are absent in undiffer evenly spaced osteoclast-like giant cells entiated carcinomas. The mononuclear cells show immunore Undifferentiated carcinoma, spindle and activity for cytokeratin and epithelial giant cell type. The tumour is composed of sheets of round cells with vesicular nuclei and prominent nucleoli that occasionally con tain cytoplasmic mucin. The fourth variant consists of well defined nodules or lobules of neo plastic cells superficially resembling breast carcinoma. The overlying biliary epithelium is non-neo sarcomatous component with osteoid formation. Carcinoma 209 component, which helps to distinguish association with the Peutz-Jeghers syn including somatostatin, pancreatic carcinosarcomas from spindle and giant drome or with Gardner syndrome polypeptide, and gastrin have been cell carcinomas. These ithelial neoplasia, but larger adenomas Adenocarcinomas can be divided into benign tumours are not associated with may have high-grade changes or foci of well, moderately, or poorly differentiated lithiasis. The diagnosis of well differentiat According to their pattern of growth, they most adenomas develop a pedicle and ed adenocarcinoma requires that 95% of are divided into three types: tubular, pap project into the lumen. Cytologically, extend into or arise from Rokitansky ately differentiated adenocarcinoma 40 they are classified as: pyloric gland type, Aschoff sinuses, a finding that should not to 94% of the tumour should be com intestinal type, and biliary type. Undiffer al type adenomas are more common in benign tumour is composed of tubular entiated carcinomas display less than the extrahepatic bile ducts . It consists of tubular Precursor lesions benign tumour composed of closely glands lined by pseudostratified colum Adenoma packed short tubular glands that are sim nar cells with elongated hyperchromatic Adenomas are benign neoplasms of ilar to pyloric glands. Early lesions nuclei, and high-grade dysplastic glandular epithelium (intraepithelial neo appear as well demarcated nodules changes are frequent. The glands lack plasia) that are typically polypoid, single embedded in the lamina propria and invasive properties and focally are and well-demarcated. They are composed of lobules that con adenomatous epithelium may extend into There is a wide age range; although tain closely packed pyloric-type glands, the Rokitansky-Aschoff sinuses, a finding mostly a disease of adults rare gallblad some of which may be cystically dilated. They are more common in the cuboidal with vesicular or hyperchromat endocrine cells are usually mixed with gallbladder than in the extrahepatic bile ic nuclei and small nucleoli and variable the columnar cells. Nodular frequently, peptide hormones have been bladders removed for cholelithiasis or aggregates of cytologically bland spin identified in the endocrine cells by chronic cholecystitis. A small proportion dle cells with eosinophilic cytoplasm but immunohistochemistry. Hyperplasia of of adenomas progress to carcinoma {42, without keratinization or intercellular metaplastic pyloric type glands is often 909, 967}. Adenomas are often small, asympto {984, 1361} are present in about 10% of Papillary adenoma, intestinal type. This matic, and usually discovered incidental the cases, whereas frank squamous benign tumour consists predominantly of ly during cholecystectomy, but they can metaplasia is exceedingly rare. Paneth papillary structures lined by dysplastic be multiple, fill the lumen of the gallblad cells and endocrine cells are often pres cells with an intestinal phenotype. By immunohistochemistry, serotonin adenomas, which usually arise in a back adenomas of the gallbladder occur in and a variety of peptide hormones ground of pyloric gland metaplasia, may B A Fig. In a series of five intestin the term tubulo-papillary adenoma is lary adenomas, that may involve exten al type papillary adenomas of the gall applied. Two subtypes are recognized: sive areas of the extrahepatic bile ducts bladder, one progressed to invasive car one is composed of tubular glands and and even extend into the gallbladder and cinoma . The predominant cell is papillary structures similar to those of intrahepatic bile ducts. The disease columnar with elongated hyperchromatic tubulovillous intestinal adenomas; the affects both sexes equally. The cells are pseudostratified, mitotically similar to pyloric glands and papillary Complete excision of the multicentric active, and indistinguishable from those structures often lined by foveolar epithe lesions is difficult and local recurrence is of villous adenomas arising in the large lium. Rarely, tubulo-papillary ous papillary structures as well as com same type of epithelium, but represent adenomas arise from the epithelial plex glandular formations. Because ing less than 20% of the tumour, may also invaginations of adenomyomatous hyper severe dysplasia is often present, papillo be found. Also present are goblet, Paneth, Other benign biliary lesions lesion as a form of low-grade multicentric and serotonin-containing cells. Papil the endocrine cells are immunoreactive resemble their intrahepatic counterparts lomatosis has a greater potential for for peptide hormones. This mas are seen predominantly among Intraepithelial neoplasia (dysplasia) lesion consists predominantly of papil adult females and are usually sympto If intraepithelial neoplasia is found, multi lary structures lined by cells with a biliary matic. Cholecystectomy is a consists of papillary structures lined by obstructive jaundice or cholecystitis-like curative surgical procedure for patients tall columnar cells, which except for the symptoms. More common in the extra with in situ carcinoma or with carcinoma presence of more cytoplasmic mucin hepatic bile ducts than in the gallblad extending into the lamina propria . Endocrine or Paneth neoplasms that contain mucinous or neoplasia of the gallbladder reflects that cells are not found. Only mild dysplastic serous fluid and are lined by columnar of invasive carcinoma. In situ or invasive epithelium reminiscent of bile duct which carcinoma of the gallbladder is carcinoma has not been reported in or foveolar gastric epithelium . This is Occasionally endocrine cells are pres countries in which this tumour is spo the rarest form of adenoma of the gall ent. The stroma gallbladders with lithiasis has varied from are examples of hyperplasia secondary also shows variable fibrosis. Papillo of uniformity in morphological criteria glands and papillary structures each matosis is a clinicopathological condition and sampling methods. Intraepithelial between normal-appearing columnar neoplasia is usually not recognized on cells and intraepithelial neoplasia is seen macroscopic examination because it in nearly all cases. In general, the cell often occurs in association with chronic population of dysplasia is homogeneous, cholecystitis. The mucosa may appear unlike the heterogeneous cell population granular, nodular, plaque-like, or trabec of the epithelial atypia of repair. The papillary type of intraepithe spread involvement of the mucosa by lial neoplasia usually appears as a small, intraepithelial neoplasia often occurs. For cauliflower-like excrescence that projects this reason, we have suggested that into the lumen and can be recognized on some, if not most, invasive carcinomas of close inspection. In the late two types of intraepithelial neoplasia are p53 occurs in some lesions . Reactive epithelial ical picture is that of back-to-back glands being more common. Some show Intraepithelial neoplasia usually begins cuboidal cells, atrophic-appearing epithe distinctive papillary features with small on the surface epithelium and subse lium, and pencil-like cells are present.
Contamination anti viral apps order prograf cheap online, disinfection antiviral used for h1n1 generic prograf 1mg overnight delivery, and cross-colonization: are hospital surfaces reservoirs for nosocomial infection Growth and survival of bacteria implicated in sudden infant death syndrome on cot mattress materials hiv infection rate in us purchase genuine prograf online. Long-term survival of vancomycin-resistant Enterococcus faecium on a contaminated surface hiv infected macrophages cheap prograf 5mg with mastercard. Survival of bacteria under dry conditions; from a viewpoint of nosocomial infection hiv infection signs and symptoms effective 1mg prograf. Survival of Acinetobacter baumannii on dry surfaces: comparison of outbreak and sporadic isolates hiv infection kinetics order generic prograf. Adherence and survival properties of an epidemic methicillin-resistant strain of Staphylococcus aureus compared with those of methicillin-sensitive strains. Contamination of hands with methicillin-resistant Staphylococcus aureus after contact with environmental surfaces and after contact with the skin of colonized patients. Quantitative detection of Clostridium difficile in hospital environmental samples by real-time polymerase chain reaction. Isolation of Clostridium difficile from the environment and contacts of patients with antibiotic-associated colitis. Acquisition of nosocomial pathogens on hands after contact with environmental surfaces near hospitalized patients. Environmental contamination due to methicillin resistant Staphylococcus aureus: possible infection control implications. Clinical and molecular epidemiology of sporadic and clustered cases of nosocomial Clostridium difficile diarrhea. Control of a clonal outbreak of multidrug-resistant Acinetobacter baumannii in a hospital of the Basque country after the introduction of environmental cleaning led by the systematic sampling from environmental objects. Epidemiology and control of an outbreak of vancomycin-resistant enterococci in the intensive care units. Control and outcome of a large outbreak of colonization and infection with glycopeptide-intermediate Staphylococcus aureus in an intensive care unit. Evidence that hospital hygiene is important in the control of methicillin-resistant Staphylococcus aureus. Characterization of a hospital outbreak of imipenem-resistant Acinetobacter baumannii by phenotypic and genotypic typing methods. Environmental cleaning intervention and risk of acquiring multidrug-resistant organisms from prior room occupants. Significant impact of terminal room cleaning with bleach on reducing nosocomial Clostridium difficile. Use of hypochlorite solution to decrease rates of Clostridium difficile-associated diarrhea. Preventing the transmission of multidrug resistant organisms: modeling the relative importance of hand hygiene and environmental cleaning interventions. Disinfection of fabrics and carpets artificially contaminated with calicivirus: relevance in institutional and healthcare centres. Comparison of the efficacy of a hydrogen peroxide dry mist disinfection system and sodium hypochlorite solution for eradication of Clostridium difficile spores. Assessment of materials commonly utilized in healthcare: implications for bacterial survival and transmission. A quantitative study of the survival of two species of Candida on porous and non-porous environmental surfaces and hands. Persistent contamination of fabric-covered furniture by vancomycin-resistant enterococci: implications for upholstery selection in hospitals. Role of healthcare apparel and other healthcare textiles in the transmission of pathogens: a review of the literature. Assessment of materials commonly utilized in health care: implications for bacterial survival and transmission. Outbreak of invasive group A Streptococcus infection: contaminated patient curtains and cross-infection on an ear, nose and throat ward. Effectiveness of improved hydrogen peroxide in decontaminating privacy curtains contaminated with multidrug-resistant pathogens. Hospital privacy curtains are frequently and rapidly contaminated with potentially pathogenic bacteria. Carbapenem-resistant Acinetobacter and role of curtains in an outbreak in intensive care units. Analysis of the recent cluster of invasive fungal sinusitis at the Toronto Hospital for Sick Children. Nosocomial outbreak of Aspergillus fumigatus infection among patients in a renal unit Nosocomial outbreak caused by Scedosporium prolificans (inflatum): four fatal cases in leukemic patients. Chemoprophylaxis for candidosis and aspergillosis in neutropenia and transplantation: a review and recommendations. Interaction of granulocytopenia and construction activity as risk factors for nosocomial invasive filamentous fungal disease in patients with hematologic disorders. An outbreak of invasive aspergillosis among allogeneic bone marrow transplants: a case-control study. A pilot study of the measurement and control of deep dust, surface dust, and lead in 10 old carpets using the 3-spot test while vacuuming. Mold prevention strategies and possible health effects in the aftermath of hurricanes and major floods. Presented at: 23rd European Congress of Clinical Microbiology and Infectious Diseases; 2013 April 27-30; Berlin, Germany. Helsinki, Finland: Laurea University of Applied Sciences; 2010 [cited 2016 Feb 2]. Isolation frequency of Candida present on the surfaces of mobile phones and hands. Effectiveness of stringent decontamination of computer input devices in the era of electronic medical records and bedside computing: a randomized controlled trial. Surface microbiology of the iPad tablet computer and the potential to serve as a fomite in both inpatient practice settings as well as outside of the hospital environment. Guidance document safety and efficacy requirements for hard surface disinfectant drugs [Internet]. Respiratory symptoms and skin irritation among hospital workers using a new disinfectant product Pennsylvania, 2015;. Infection prevention and control of epidemic and pandemic-prone respiratory infections in health care. The effect of interfering substances on the disinfection process: a mathematical model. Hospital management of Clostridium difficile infection: a review of the literature. Quaternary ammonium disinfectant issues encountered in an environmental services department. Modern technologies for improving cleaning and disinfection of environmental surfaces in hospitals. Disinfectant contaminated with Klebsiella oxytoca as a source of sepsis in babies. Environmental contamination by multidrug resistant microorganisms after daily cleaning. Bacterial growth in an in-use hospital-grade quaternary ammonium-based disinfectant. The value of ready-to-use disinfectant wipes: compliance, employee time, and costs. Ability of cleaning-disinfecting wipes to remove bacteria from medical device surfaces. Efficacy of commercially available wipes for disinfection of pulse oximeter sensors. Effectiveness of common healthcare disinfectants against H1N1 influenza virus on reusable elastomeric respirators. Standardized, app-based disinfection of iPads in a clinical and nonclinical setting: comparative analysis. Poorly processed reusable surface disinfection tissue dispensers may be a source of infection. Identical Achromobacter strain in reusable surface disinfection tissue dispensers and a clinical isolate. Lesser-known or hidden reservoirs of infection and implications for adequate prevention strategies: where to look and what to look for. Removing bacteria from hospital surfaces: a laboratory comparison of ultramicrofibre and standard cloths. Microfiber cloths reduce the transfer of Clostridium difficile spores to environmental surfaces compared with cotton cloths. Health care workers use disposable microfiber cloths for cleaning clinical equipment. Performance of ultramicrofibre cleaning technology with or without addition of a novel copper-based biocide. Assessing the efficacy of different microfibre cloths at removing surface micro-organisms associated with healthcare-associated infections. Evaluation of the decontamination efficacy of new and reprocessed microfiber cleaning cloth compared with other commonly used cleaning cloths in the hospital. Reduction in nosocomial infection with improved hand hygiene in intensive care units of a tertiary care hospital in Argentina. Association between use of hand hygiene products and rates of health care-associated infections in a large university hospital in Norway. Effectiveness and limitations of hand hygiene promotion on decreasing healthcare-associated infections. Impact of a hospital-wide hand hygiene initiative on healthcare-associated infections: results of an interrupted time series. Time-series analysis of the relationship of antimicrobial use and hand hygiene promotion with the incidence of healthcare-associated infections. Handwashing practices in an intensive care unit: the effects of an educational program and its relationship to infection rates. Electronic monitoring and voice prompts improve hand hygiene and decrease nosocomial infections in an intermediate care unit. Comparative efficacy of alternative hand-washing agents in reducing nosocomial infections in intensive care units. Failure of gloves and other protective devices to prevent transmission of hepatitis B virus to oral surgeons. Efficacy of handrubbing with alcohol based solution versus standard handwashing with antiseptic soap: randomised clinical trial. Routine practices and additional precautions for preventing the transmission of infection in health care. Prevention of irritant contact dermatitis among health care workers by using evidence-based hand hygiene practices: a review. Nosocomial acquisition of methicillin-resistant Staphylococcus aureus during an outbreak of severe acute respiratory syndrome. Association of contaminated gloves with transmission of Acinetobacter calcoaceticus var. Reduction in acquisition of vancomycin-resistant Enterococcus after enforcement of routine environmental cleaning measures. Importance of the environment in meticillin-resistant Staphylococcus aureus acquisition: the case for hospital cleaning. Evaluation of hospital room assignment and acquisition of Clostridium difficile infection. Role of environmental cleaning in controlling an outbreak of Acinetobacter baumannii on a neurosurgical intensive care unit. An integrated approach to hospital cleaning: microfibre cloth and steam cleaning technology [Internet]. Essential resources for effective infection prevention and control programs: A matter of patient safety a discussion paper [Internet]. Cleaning up; how hospital outsourcing is hurting workers and endangering patients. Contracting out hospital support jobs: the effects of poverty wages, excessive workload, and job insecurity on work and family life. The pains of privatization: how contracting out hurts health support workers, their families, and health care [Internet]. The impact of enhanced cleaning within the intensive care unit on contamination of the near-patient environment with hospital pathogens: a randomized crossover study in critical care units in two hospitals. Working relationships of infection prevention and control programs and environmental services and associations with antibiotic-resistant organisms in Canadian acute care hospitals. Risk reference sheet: Infection control healthcare acquired infections [Internet]. The influence of patient room type, cleaning procedure, and isolation precautions on room cleaning times in Canadian acute care hospitals. The time spent cleaning a hospital room does not correlate with the thoroughness of cleaning.
Prograf 5 mg sale. Ghanaian Pastor Who Has HIV/AIDS With Wife Shares Sad Story Mentions HIV Victims.